
High-profile shootings and student suicides have made mental health issues on college campuses a major national issue. College students are usually the focus of this conversation, while little attention beyond anecdotal accounts has been paid to faculty with mental health issues. In response to this lack of broad-scale research, a first-of-its-kind cross-institutional survey of faculty with mental disabilities was conducted. Respondents self-identified as faculty with mental disabilities, mental illness or mental-health histories. Results from 267 respondents indicated that nearly 70% had no or limited familiarity with accommodations, and even fewer used them (87%). A majority of respondents (62%) disclosed to at least one person on campus, primarily colleagues (50%) and department chairs (21%). Respondents felt most supported by spouses/significant others (75% very or extremely supported) and friends (51%) rather than colleagues (29%) and supervisors (25%). In our discussion of these findings, we offer suggestions for practice that will improve environments, rather than focusing on case-by-case "fixes" for those who disclose. We also suggest directions for further research into this topic, which is frequently mentioned (in both scholarly and popular publications) but rarely investigated systematically or on a wide scale.
Disclosure of Mental Disability by College and University Faculty: The Negotiation of Accommodations, Supports, and Barriers1
In 2015, Peter Railton announced in a speech to the American Philosophical Association that he has depression and, before his speech, had hidden it for decades: "I couldn't say it. I couldn't say, 'Look, I'm dying inside. I need help'" (Railton, 2015). Other high-profile mental-health disclosures by faculty have come from Kay Redfield Jamison, a professor of psychology with bipolar disorder (1995), and Elyn Saks, a professor of law with schizophrenia (2007). Meanwhile, still more disclosures have appeared through small case studies or personal essays (see, for example, Avinger, Croake & Miller, 2007; Brottman, 2007; Hogan, 2007; Jago, 2007; Pryal, 2014; Skogen, 2012; Snitker, 2007; Tsipursky, 2015; White, 2007). These individual revelations bring attention to the fact that little is known about the experiences of faculty with mental disabilities as a group.2 How often do they disclose, and under what circumstances? What supports do they draw upon? What barriers must they negotiate? For disabled faculty, "rarely are standard policies in place," and, since the Office of Disability Services may work only with students, faculty must negotiate their access needs among "scattered units" at their schools (Smith & Andrews 2015, p. 1522). This problem is further complicated when faculty members feel reluctant to disclose in the first place, as is often the case with mental disabilities.
In an effort to begin creating a more systematic body of knowledge, we conducted an anonymous survey of faculty who self-identified as having mental-health histories.3 We designed the survey with the following research questions in mind:
- How often do faculty with mental disabilities disclose their disabilities?
- To whom do they disclose (if they do), and why do they choose those people/forums for disclosure?
- What accommodations do faculty with mental disabilities request? If they do not request accommodations, why not?
- What accommodations do faculty with mental disabilities consider most useful, or (if they do not receive accommodations) do they imagine would be most useful?
- What supports do faculty with mental disabilities draw upon, and what barriers do they report negotiating?
As noted in the following review of research, most of the available literature comes from individual accounts or small studies. That information, placed alongside the few larger studies that are available, points to the key issues we focused on in our survey: disclosure, accommodation, institutional supports, and institutional barriers.
Current Research on Faculty with Mental Disabilities
Research on faculty members with mental disabilities has appeared mostly in the form of small-scale studies and first-person accounts. Many of these smaller studies and first-person accounts appear in anthologies (see, for example, Myers, 2007; Vance, 2007; LeFrançois, Menzies & Reaume, 2013). Some studies have focused on faculty with disabilities generally; these may be institution-specific ("Faculty with Disabilities Survey," 2011; Shigaki et al., 2012), discipline-specific (Horton & Tucker, 2013), or may look at a particular phenomenon, such as requests for accommodation (Baldridge & Viega, 2006; Baldridge & Swift, 2013). Specialized studies focusing exclusively on faculty with mental disabilities are rare. One such study, from the UK Guardian, surveyed 2,500 academics and found that over half of respondents with mental-health issues chose not to disclose their disabilities at work; one respondent is quoted as saying, "It never even dawned on me to seek help or even to see my situation as something requiring external help" (Thomas, 2014, n.p.).4 More recently, a special issue of The Canadian Geographer focused on "Cultivating an Ethic of Wellness in Geography," with the issue editors stating:
A wider and integrated approach to health and wellbeing in the academy is needed; an approach that considers not only the wider world in which the crisis on campuses is occurring, but also the micro-scale and subtle relationships that are capable of much harm, and the often unrecognized groups within our communities that suffer, often silently, and sometimes from multiple and overlapping forms of distress. (Mullings, Peake & Parizeau, 2016, p. 166)
In the U.S., mental-health issues in higher education, more often associated with students but occasionally with faculty, may be tied to fears about mass shootings. These fears are often discussed in terms of race as well as mental illness (Watts and Erevelles, 2004; Brandzel and Desai, 2008).
Taken as a whole, the existing literature about faculty with mental disabilities suggests the following:
- Faculty with mental disabilities often avoid the "official" route of arranging accommodations through their employers, instead handling their accommodation needs informally or privately.
- Lack of connection with institutional support may occur because faculty are unable to determine which office or person is supposed to handle faculty accommodation requests.
- Faculty with mental disabilities may be reluctant to seek accommodations because they infer that having such disabilities will be judged as a sign of unfitness for their jobs.
Our survey5 sought to substantiate these "hunches" by conducting a study on a wider scale. We also sought to learn more about the circumstances under which faculty disclosed and/or requested accommodations (or chose not to do so); how they identified themselves vis-à-vis mental-health diagnoses; and what supports and barriers they experienced in the course of their jobs. The survey asked a detailed series of questions about disclosure: why respondents did or did not disclose or seek accommodations on the job; to whom they disclosed; and how they felt about those encounters. We designed the survey to go into detail about the contextual factors surrounding disclosures because prior investigations, especially those in the Disability Studies literature, indicate that disclosure of disability is a highly complex endeavor—an issue seldom acknowledged in studies from other disciplines.
What Does It Mean to "Disclose" Disability?
Within Disability Studies, theories of disclosure as a complex and multi-faceted rhetorical process have been building for over a decade. An early argument, from philosopher Cal Montgomery in Ragged Edge, suggested:
Dismissing that which is unfamiliar to us as "invisible" (and suggesting that it cannot be discerned rather than that we have not learned to discern it) is another way of throwing the responsibility for social justice back on the individual who carries the burden of injustice. (Montgomery, 2001, n.p.; emphasis added)
In other words, the "visibility" metaphor implies accountability: it assumes that the disabled person who is "invisible" is responsible for making himself visible, or discernible. When we make this assumption, responsibility for alleviating injustice is placed upon the person suffering the injustice in the first place. Oppressed persons should not bear the burden of educating and reforming their oppressors, and yet, that is what the visible/invisible metaphor asks of disabled people.
Montgomery's ideas paved the way for influential articles including Ellen Samuels's "My Body, My Closet: Invisible Disability and the Limits of Coming-out Discourse" (2003) and Tobin Siebers's "Disability as Masquerade" (2004). Both of these articles argued that the act of disabled passing reveals the instability of the category "disabled" in the first place, while also disrupting the assumption of a passive disabled person: "The passing subject may be read not as an assimilationist victim but as a defiant figure" (Samuels, 2003, p. 243). This turn away from simple metaphors of "visibility" or "coming out" also impacted the tendency to refer to "the closet," and was explored in later studies such as Margaret Price's Mad at School (2011), which suggested replacing the metaphor of the closet with the image of a "hall of mirrors" (p. 179). In similar fashion, Annie Irvine's (2011) study of mental-health disclosure in the workplace argues that it makes more sense to consider a "continuum of mental health" (p. 187) rather than to adhere to strict labels of disabled/nondisabled, in order to account for the many contextual factors that construct the process of disclosure. More recently, Stephanie Kerschbaum's (2014) "On Rhetorical Agency and Disclosing Disability in Academic Writing" has moved forward from the general acknowledgement that visibility and closeting are inadequate metaphors, arguing for a theory of disability disclosure as an emergent, negotiated process involving speakers/writers, their audiences, and the settings in which their interactions unfold. A review of mental-health disclosure research by Brohan et al. (2012) confirms that, upon analysis of 48 studies focusing on workplace disclosure, it is more accurate to describe disclosure as occurring through a number of dimensions rather than adhering to a "dichotomous view" (p. 12).
The growing awareness of the complexity of disability disclosure sometimes overlaps with scholarship in critical race studies and queer/gender studies. Some works, including Brune and Wilson (2013) and Dawkins (2012), have brought these areas of study together, resulting in a more nuanced understanding of the phenomenon called passing, which is not always a clear-cut choice or decision. For example, Dawkins (2012) noted that, "passers are [conventionally] expected to fail and suffer at their own hands rather than challenge collective notions of racial identity and typecasting in popular culture" (p. 126); in other words, passers in the conventional imagination have caved to the status quo rather than challenged it. Yet, as Dawkins's and many other accounts have shown, disability passing may be a trickster strategy, one that disrupts the status quo through subversive means (see Brueggemann, 1999; Samuels, 2003). Moreover, a person may pass against their will: Siebers (2008) argued that "Closeting involves things not merely concealed but difficult to disclose—the inability to disclose is, in fact, one of the constitutive markers of oppression" (p. 97). In other words, a disabled person may remain "invisible," or be mis-recognized, despite deliberate efforts to be apparent.
Although Disability Studies and other minority-studies disciplines have explored the rhetorical complexity of disclosure, higher-education literature often treats disclosure as an easily identifiable, singular event. For example, the American Association of University Professors' "Accommodating Faculty Members Who Have Disabilities" (2012) states that "it is incumbent on the individual [disabled faculty member] to bring the matter to the attention of appropriate institutional authorities" (p. 3), but does not discuss the many reasons this might be a fraught endeavor; indeed, that even what it might mean to "bring attention" to one's disability might be difficult to figure out (Kerschbaum et al., 2013). Rochelle Skogen in the Harvard Educational Review (2012) takes a similarly straightforward view, reporting that "in spite of what may await me after disclosure [through this article's publication], the process of writing and sharing my story has, in many ways, emancipated me from the stigma of mental illness" (p. 508). However, this understanding of disclosure—as an easily identifiable, even emancipatory event—does not reflect the more nuanced understanding that has emerged in Disability Studies and other minority-studies fields over the past 15 years.
Instead of being a single occurrence that leads to subsequent understanding, disability disclosure is better understood as an ongoing rhetorical process in which faculty members repeatedly need to address their disability for various audiences, across many different contexts (Kerschbaum et al., 2013). Moreover, disability disclosure is inevitably entangled with other identity markers, including race, gender, academic rank, and so forth. Unfortunately, higher-education policy and practice usually operate according to an individual model, which assumes that individuals must disclose, negotiate accommodations, and thereby obtain access (Venville, Street & Fossey, 2014). The notion of universal or participatory design—in which "access is conceived not as attaching to a disabled person but to the broad physical, social, and intellectual environment of the university" (Samuels in Kerschbaum et al., 2013, n.p.)—is difficult to find in practice, despite its long-standing theoretical recognition across multiple disciplines (see Dolmage, 2008, 2015; Glass, Meyer and Rose, 2013; Hamraie, 2013; Titchkosky, 2011).
Methods
This is the first survey to sample a large group of self-identified faculty with mental-health histories across a range of institutions in the United States. We were aware when designing the survey that this group had not been sampled on a broad scale in prior research, and we were also aware that stigma might be a factor in participants' willingness to respond (see Venville, Street & Fossey, 2014). For these reasons, the survey was designed to be anonymous, with no possibility of identification or follow-up.6 Participants were recruited by posting announcements on listservs across a range of disciplines, and by direct emails to human resource departments, disability-service offices, and professional associations. This approach was used in a similarly novel study of the experiences of U.S. college students with mental illnesses (Salzer et al., 2008; Salzer, 2012). Some individuals who received our call for participants passed it along to members-only listservs (for example, the faculty within a particular department or college).
The information in recruitment messages directed potential participants to a site where they obtained additional information about the survey, including the following:
For the purposes of this survey, person with mental disability means someone who has received mental-health care and/or a mental-health diagnosis. You do not have to identify as 'disabled' to participate in this survey; you may alternatively identify as a mental-health services consumer, a psychiatric survivor, a person with mental illness, a psychocrip, or simply someone with your particular diagnosis.
The study received IRB approval from the universities where the two lead authors are employed. A total of 267 surveys were completed and analyzed using SPSS 22.0.
The survey was divided into four sections: Demographic information; Mental health background; Disclosure and work modifications; Barriers and supports. The survey's language was designed to achieve both inclusivity and clarity. The survey was accessible to screen readers and laid out in a predictable visual pattern; in other words, we adhered to established standards of Web accessibility. The survey was also designed to maximize respondent autonomy and minimize potential distress from questions that might bring up painful experiences. For example, in addition to being given a list of diagnostic labels that they felt best described their mental health condition, participants were offered the option to write in their own identifications "if you identify your mental health in terms other than, or in addition to, diagnostic labels."
Understanding that mention of hospitalization might be traumatizing, we carefully considered whether to include a question about respondents' previous number of psychiatric hospitalizations. We chose to keep it, in order to gain a better understanding of the ways that participants' mental-health issues affected their lives, but included a content-warning note in the introductory page of the survey to indicate that this question would be coming:
This survey will ask about topics including diagnoses, medication (although we do not ask what specific medications you may take), hospitalizations, relations with co-workers, and experiences of disclosure at work.
The survey was vetted by colleagues in a range of disciplines and then piloted among a group of 10 people (both with and without mental-health disabilities) to test its usability and accessibility. Feedback from these sessions was incorporated into the survey's final form.
Results
Demographic characteristics
The demographic section asked participants to describe themselves in five areas: faculty rank, institution type, gender, race, and primary diagnosis. Respondents were able to select more than one category for institution type, gender, and race. Over half of respondents (66.2%, N=176) reported being employed as assistant, associate, or full professors, with the largest sub-group being assistant professors (29.3%, N=78). A large minority (33.5%, N=89) reported employment as non-tenure-track faculty, with the largest sub-group of these being faculty on contracts of less than one year (16.5%, N=44). The most common institutional types reported were universities granting graduate degrees (73.3%, N=195); four-year undergraduate institutions (18.0%, N=48); and community colleges (7.9%, N=21), with historically Black colleges/universities (HBCUs) and specialized schools represented in small numbers.
Women responded to the survey in the greatest numbers: 69.7% of respondents (N=186) identified themselves as women, 29.2% (N=78) as men, and 4.4% (N=12) as genderqueer, transgender, transsexual, or other. White respondents were also a large majority, 93.3% (N=249), with participants of color identifying themselves as Black and/or African American (3.7%, N=10), Asian (2.6%, N=7), Latino and/or Hispanic (1.5%, N=4), American Indian (1.5%, N=4), and other (1.5%, N=4). The most common primary diagnosis reported was depression (46.8%, N=125), followed by anxiety (37.5%, N=100), bipolar disorder (8.2%, N=22), and attention-deficit/hyperactivity disorder (4.5%, N=12).
We offer these demographic characteristics in order to be as transparent as possible about the survey's respondents. The majorities represented in some groups, including white people and those on the tenure track, merits further questioning and research; see "Discussion."
Familiarity and Requests for Accommodations
All participants were asked, "How familiar are you with accommodations that you may be entitled to under the law?" and presented with a range of possible responses from "not familiar at all" to "extremely familiar." Almost half of respondents (44.9%, N = 120) reported that they were "not familiar at all," with almost a quarter (24.3%, N = 65) reporting that they were "slightly familiar." Only 7.1% (N = 19) reported that they were "extremely familiar" with accommodations to which they were entitled. Approximately 13.1% (N = 35) of respondents indicated that they had requested accommodations, while a large majority (86.9%, N = 232) indicated that they had not.
The large group of respondents who indicated that they had never requested accommodations related to their mental disabilities were then asked "Why not?" and given a list of possible reasons along with an option to add an additional reason not listed. Participants were able to select more than one option, if applicable. The most common response was "Do not need them" (50.0%, N=116), followed by "Was not aware that they were available" (33.6%, N=78), "Feeling that it's not other peoples' business" (30.6%, N=71), and two categories suggesting potential outcomes—"Possibility that the request would affect tenure/promotion" (25.0%, N=58) and "Possibility that people might avoid me or treat me badly" (21.6%, N=50). No respondents selected the option "Cannot acquire necessary documentation."
Open-ended responses ranged widely: some respondents stated that they feel mental health is a personal issue; some elaborated on their fear of negative outcomes; some stated that they simply felt they didn't need accommodations, or that accommodations already given to everyone in the office (such as flexible scheduling) met their needs. Fear of stigma was a significant theme that ran throughout many of the open-ended responses. One participant wrote, succinctly, "One word—STIGMA"; another wrote, "FEAR of losing [a]ll credibility." Another elaborated more fully: "I do not think that the risk of serious reprisal is high, but I have seen a colleague with a serious mental health issue subjected to constant gossip, originating with administrators, and I believe such would seriously damage my ability to work."
Disclosure
All participants were asked, "To whom at your workplace have you disclosed your disability?" Of the 267 participants, 62% (N=165) indicated they had disclosed to at least one person. Respondents were able to select more than one option, if applicable, for this item. About half (49.8%, N = 133) of respondents indicated that they had disclosed to a colleague, 21.0% (N=56) disclosed to their Department Chair, and 19.5% (N=52) disclosed to students. Much smaller percentages of respondents indicated that they had disclosed to a dean or provost (6.4%, N=17) or to the Office of Disability Services (3.7%, or N=10).
About a third of respondents to this question (34.1%, N=91) selected "No one" in response. This group was then asked to specify why they had chosen not to disclose their mental disability to anyone at their workplace. Again, it was possible to select more than one option, if applicable. The largest percentage of this group selected the responses "Feeling that it's not other peoples' business" (61.5%, N=56) and "Feeling that it's not relevant to my work" (50.5%, N=46). The next largest percentages of selected responses had to do with possible negative outcomes: "Possibility that people might avoid me or treat me badly" (46.2%, N=42), "Possibility that the request would affect tenure/promotion" (31.9%, N=29), and "Possibility of not having contract renewed" (26.4%, N=24). Smaller, but still significant, selections within this non-disclosing group were the options "Possibility of losing job" (16.5%, N=15) or "Possibility that the request would affect salary or benefits" (13.2%, N=12). As with the previous questions, this one included a space for open-ended response. Again, privacy was an important theme, as was stigma. One participant brought up an interesting issue of double diagnosis:
I also have two other disabilities that are visible, so often use those as rationales for any accommodations I need for mental health issues (e.g., instead of saying "I had a bad night sleeping because of anxiety," I would say, "I was up all night with my health condition." People at work know about the other disabilities and I talk about them freely.
From this participant's response, it seems that the fear of stigma may be less for disabilities other than those pertaining to mental health. This phenomenon, called "selective disclosure" by Tara Wood (in press), has been observed in other studies of disability in higher education.
Participants who indicated that they had disclosed to someone at their workplace were asked to characterize their experiences of disclosure to each of the eight previously mentioned groups (colleague, department chair, dean or provost, office of disability services, faculty ombudsperson, office of human resources, other staff member, or students). Only respondents who indicated previously in the survey that they had disclosed their disability to a particular person or group at their workplace were included in the analysis for those categories. Frequency and percent of responses for each category are presented in Table 1. It is noteworthy that 88 out of 128 (68.7%) and 32 out of 51 (62.8%) of those who disclosed to faculty colleagues and chairs, respectively, felt it was received positively (Very, Moderately, or Slightly Positive, combined), while only 3 of the 11 individuals (27.3%) who disclosed to Human Resources personnel felt it was received positively. Of all groups, respondents felt students reacted most positively to disclosures (44 out of 49 disclosures; 89.8%).
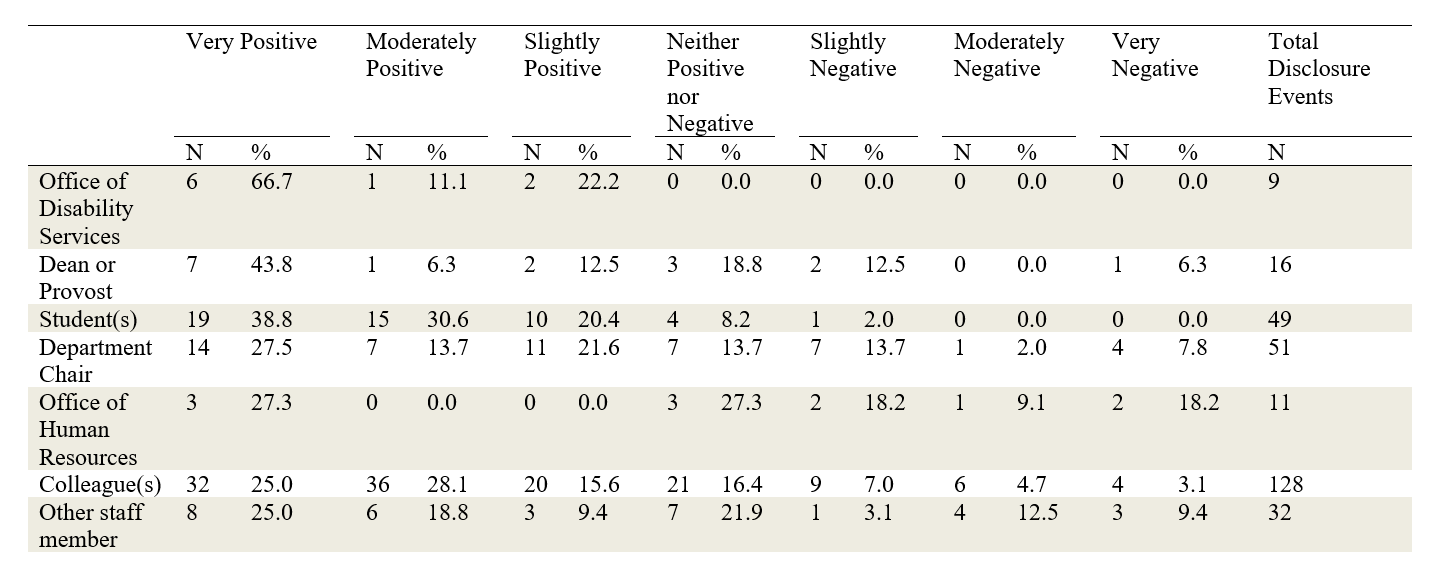
Table 1. Experience of Disclosure*
* Note: The totals for experience of disclosure to individuals and groups may not add up to the total number of respondents who indicated they disclosed to that group, as respondents who were missing 10% or more of data were excluded. While the survey provided participants with the option to report on their experiences disclosing to faculty ombudsperson, no respondents selected this option and, therefore, it is not included in the table.
Table Description: This table shows respondents' ratings of their disclosure experiences with various people and offices; the ratings range from positive to negative. The people and offices listed, which occupy the left-most column of the table, are the following: Office of Disability Services; Dean or Provost; Student(s); Department Chair; Office of Human Resources; Colleague(s); Other Staff Member. The scale, which occupies the top row of the table, includes the following range: Very Positive; Moderately Positive; Slightly Positive; Neither Positive nor Negative; Slightly Negative; Moderately Negative; Very Negative. As discussed in the body of the article, the most total reported disclosure events were made to colleagues, then department chairs and students, respectively. Among these three categories, the largest percentage of "very" or "moderately" positive disclosure events occurred with students, then colleagues and department chairs, respectively.
Support
All respondents were asked, "To what extent have the following people or groups been valuable in providing support for you at your current institution?" using a response scale from "not at all" to "extremely" indicating the degree to which they felt different people or groups were valuable in providing support at their current institution. The frequencies and percentages for each of the categories are presented in Table 2. The strongest supports were offered by spouses and significant others, with more than half of the survey respondents (52.7%, N=109) indicating that their spouse or significant other was "extremely" supportive, and another 22.2% (N=46) indicating that their spouse or significant other was "very" supportive. On the other end of the spectrum, four groups were identified by survey respondents as "not at all" supportive: their professional organization, on-campus mental health services, staff members, and supervisors.
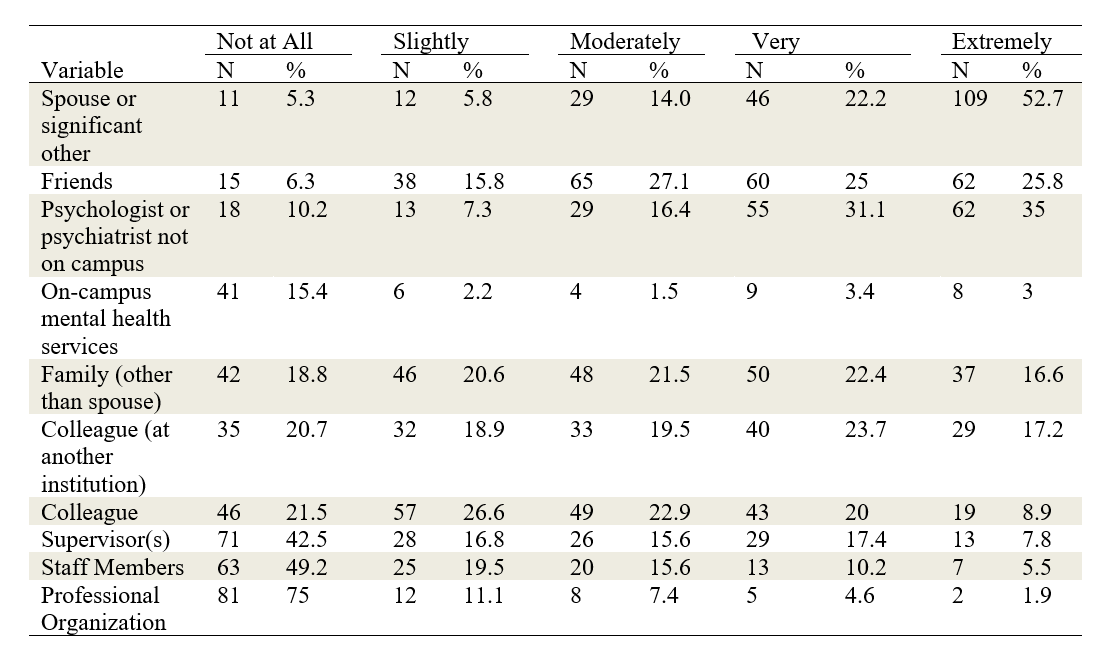
Table 2. Support at Current Institution
Table Description: This table shows respondents' ratings of how supportive they find various people or offices at or outside their institution. The people and offices, which occupy the left-most column of the table, are the following: Spouse or significant other; Friends; Psychologist or psychiatrist not on campus; On-campus mental health services; Family (other than spouse); Colleague (at another institution); Colleague; Supervisor(s); Staff Members; Professional Organization. The scale, which occupies the top row of the table, includes the following range: Not at All [Supportive]; Slightly [Supportive]; Moderately [Supportive]; Very [Supportive]; Extremely [Supportive]. As discussed in the body of the article, the strongest reported supports were spouses and significant others, followed by friends and off-campus mental-health professionals. The four groups identified by most survey respondents as "not at all" or only "slightly" supportive were their professional organizations, on-campus mental health services, staff members, and supervisors.
Discussion
We discuss our findings in terms of four assertions drawn from our data.7 Our primary findings are these:
- Most faculty with mental disabilities lack familiarity with accommodations that are available to them.
- Faculty with mental disabilities tend not to request accommodation.
- Among faculty who have disclosed their mental disabilities, a range of experiences was reported, with more instances of disclosure reported as positive than neutral or negative.
- The most important supports reported by faculty were their spouses or significant others, friends, and family members as well as colleagues on- and off-campus. The least important supports reported by faculty were their supervisors, their professional organizations, and on-campus mental health services.
Finding #1: Most faculty with mental disabilities lack familiarity with accommodations that are available to them.
A majority of respondents indicated that they were "not familiar at all" or only "slightly familiar" (69.3%, N = 185) with accommodations that might be available to them. This finding points to an issue that dominates our survey results: a general lack of institutional attention paid to faculty members with mental disabilities. As educational researcher and disability scholar Tanya Titchkosky notes in A Question of Access (2011), "disabled professors and staff members remain unimagined types" (p. 80) in the narratives of higher education, with the result that few people ask questions about how disabled faculty and staff might access institutional spaces and academic environments. The large number of participants in our study who indicated unfamiliarity with accommodations confirms theoretical arguments like Titchkosky's, as well as single-institution studies and personal accounts. It could also be the case that mental disabilities may seem especially difficult to accommodate: for example, if one has depression, it might be difficult to imagine how such a disability could be accommodated in the academic world of "relentless energy, forward-focus and able-mindedness" (Clark, 2007, p. 128).
Higher-education institutions can address the problem of unfamiliarity by establishing clear lines of communication about accommodations that are available. In some cases, this may mean creating a consistent policy where none existed before. Responses to our survey suggest that channels for providing accommodation for faculty members tend to be confusing, and are often handled on a case-by-case basis, rather than operating according to consistent guidelines. While many colleges and universities have campus disability support services, as well as legally-mandated ADA compliance officers, conversations about disability usually focus on students, not faculty. Respondents who did receive accommodations indicated that these came from a wide range of offices, including Human Resources, variously-named equity and/or diversity offices, ADA coordinators, and department chairs.
Finding #2: Faculty with mental disabilities tend not to request accommodation.
A large majority (86.9%, N = 232) of survey respondents indicated that they have not requested accommodations to their work process. This might stem in part from the lack of familiarity described above; however, the stigma attached to mental disabilities is also an important factor. Three main rationales emerge among the reasons reported for not requesting accommodations: first, that making such a request would be risky or dangerous in some way; second, that mental health issues should be private; and third, that accommodations are not needed or not relevant to respondents' work. These themes are not mutually exclusive—that is, a respondent might have selected responses according to one, two, or all three of these rationales.
A sense of risk is the most prevalent rationale in respondents' explanations of why they have not requested accommodations. Participants reported avoiding such requests because they might affect tenure and promotion, lead to avoidance or poor treatment by others, or affect factors such as salary or job security. While our results indicate that some participants report positive outcomes associated with disclosure (discussed further below), the fact that relatively few respondents have requested accommodations at all suggests that disclosures may be motivated by reasons other than making accommodation requests.
A second rationale offered was that respondents may see their mental health issues as private or personal matters, not professional ones, and avoid requesting accommodation in order to avoid having to disclose. As one faculty member put it, "As long as I can perform on the job, I want to keep my mental health issues private." This finding reinforces reports from first-person accounts that faculty often desire to keep mental-health issues private. However, as Skogen (2012) points out, such privacy can also become confining, even oppressive, on the job.
Finally, a third rationale suggests that faculty members with mental disabilities may not need accommodations, or don't see them as relevant to their work; consequently, they do not make any accommodation requests. One interpretation of this finding is that mental health issues are compatible with academic life. For example, the relative flexibility of academic schedules can be a useful means by which faculty members manage unpredictable health conditions (see, for example, Samuels, 2007). However, as numerous scholars have documented, academic life remains inhospitable in many ways to faculty members with mental health disabilities. Some open-ended responses to our survey suggest that while mental health issues do require accommodation, the accommodation is sought outside the workplace. As one respondent stated, "I feel that depression is more a personal, internal issue and that others/outsiders other than trained therapists would not be helpful if I were to disclose this issue to them," adding, "Depression is not a problem that is typically dealt with through accommodations."
For some respondents, accommodations were useful, but not tied to formal channels for officially making requests and disclosing a disability. As one participant put it, "I am able to negotiate the accommodations I need on other bases (seniority, trading out more-popular assignments for less-popular ones)." Another wrote, "I need an office with windows because I need sunlight. My office has lots of windows so I didn't have to ask for one." In some cases, faculty members with multiple diagnoses (some physical, some mental) chose to negotiate accommodation requests by disclosing only the diagnosis perceived to be less stigmatized. Wood (in press) refers to this process as "selective disclosure."
Finding #3: Among faculty who have disclosed their mental disabilities, a range of experiences was reported, with more instances of disclosure reported as positive than neutral or negative.
The most common group to whom faculty members reported disclosing a mental disability was colleagues, followed (in descending order of frequency) by "no one," a department chair, students, staff members, a dean or provost, the Office of Disability Services, and Human Resources. We see in these numbers a trend towards more informal channels for disclosure than official/institutional ones. Faculty may, for example, discuss mental health issues such as anxiety and stress with colleagues while not "officially" disclosing a specific diagnosis: as one respondent wrote, "It is one thing to talk about being stressed out in general terms and get support for that, another to provide details about anxiety, depression, mental paralysis." Because a large number of those who reported disclosing did so with colleagues (128 out of the 165 who disclosed, or 78%), it seems that selected peers are an important source of support for faculty with mental disabilities. Overall, these findings indicate a trend toward disclosures to peers, staff members, or students (N=209 out of 296 disclosure events; 71%), rather than to people higher up in the academic hierarchy, including department chairs, deans, provosts, and bureaucratic entities such as Human Resources (N=87 out of 296 disclosure events; 29%).
While many respondents reported fears associated with disclosing, when they were asked to describe their experiences of disclosing, more instances of disclosure were positive than negative: 48 reported experiences of disclosure ranged from "slightly negative" to "very negative" while 203 ranged from "slightly positive" to "very positive," including 89 instances rated as "very positive." For all groups to whom faculty members reported disclosing, the trend was toward more positive effects of disclosure, with the exception of the experiences reported by faculty who disclosed to Human Resources, although these were few, possibly in anticipation of negative experiences.
We infer from these responses that, when faculty with mental disabilities disclose, they choose their interlocutors carefully. In addition, more positive interactions seem to come from peer-to-peer or faculty-to-student interactions. This reaffirms our finding that channels of communication between faculty and administration need to become clearer and less risky; it also suggests that the general institutional attitude toward mental disabilities needs improvement.
Finding #4: The most important supports reported by faculty were their spouses or significant others, friends, and family members as well as colleagues on- and off-campus. The least important supports reported by faculty were their supervisors, their professional organizations, and on-campus mental health services.
Responses to our survey indicate a broad range of supports available to faculty as well as varying assessments of that support. However, personal supports—a spouse or significant other, friends, family members and colleagues, both at their current institution and elsewhere—are among the most important elements of faculty members' support networks, while professionally-affiliated networks such as supervisors, professional organizations, and on-campus mental health services were given overall lower support ratings. More research is needed to understand the nature of these support networks and the different kinds of support that faculty members with mental disabilities need. One point does bear repeating, however: the stigma attached to mental disability seems to make many faculty reluctant to discuss their mental-health issues, with the consequence that their supervisors and colleagues may not have opportunities to be supportive. When the attitude toward mental disability is uncertain or unclear, faculty members may be more conservative with regard to sharing their mental disabilities with others. Wider attention to such issues among faculty—that is, systemic attention to making workplaces more accessible for mental disabilities—is a necessary step toward reducing the stigma associated with such disabilities.
Study Limitations
The main limitation of this study is the extent to which our survey respondents may or may not be representative of all faculty with mental disabilities. There is no list of such faculty or primary organization to which they belong, so certain high-response-generating survey methods could not be used. Therefore, an attempt was made to circulate information about the survey through as many electronic venues as possible to as diverse an audience as possible. Similar methods were used in previously published research involving college students with mental illnesses (Salzer et al., 2008; Salzer, 2012). Aware of the general bias toward centering whiteness in research on mental-health issues, we made specific efforts to reach out to faculty of color; for example, we sent recruitment calls to individual HBCUs, asking contacts at these schools to distribute the call for participants.
We cannot assess whether we obtained a representative sample by diagnosis, as no such data exist about faculty, although the large percentage of respondents with depression is consistent with the prevalence of depression relative to other mental health conditions. It appears that we likely have an over-representation of respondents who are women, as did the UK Guardian survey (Thomas, 2014), which obtained approximately the same percentage of female respondents. Our respondent sample also under-represents faculty of color, since a large majority of respondents are white. It is imperative that future research, including our own, move forward from these initial findings to explore in more detail the intersectional dynamics of race, gender, class, age, rank, and other factors as they operate for faculty with mental disabilities. See the next section for further discussion of possibilities for future research.
Conclusion: Wondering Forward
The results from our survey demonstrate that colleges' and universities' current mechanisms for accommodating faculty with mental disabilities are inadequate. Although U.S. faculty should be protected by the Americans with Disabilities Act (ADA), which explicitly includes mental disabilities, the enactment of these protections often breaks down, as faculty do not have a strong record of success in bringing suit under the ADA (Abram, 2003)—or, as prior research and the present survey show, faculty may be reluctant to request accommodation in the first place (Baldridge & Viega, 2006; Baldridge & Swift, 2013).
In many cases, faculty do not know what protections are available to them; or, even if they have a vague sense that there is some protection in place, they are not aware of the types of accommodations they could request. Moreover, procedures for requesting accommodations are often confusing, uncertain, and/or risky. While some survey respondents indicated that they do not need accommodations, many others pointed to accommodations that would improve their work lives, including items such as flexible scheduling; offices, classrooms and meeting spaces with natural light; and access to quiet spaces away from noise and distraction (see Kerschbaum, O'Shea, Price and Salzer, in press). In some cases, faculty reported not making requests because they feared stigma.
Stigma was mentioned in many participants' open-ended responses, and plays a critical role in faculty members' work lives. Members of the academic workforce—administration as well as faculty and staff—must focus not only on the needs of individual disabled people, but also on the environments and attitudes that are constructed within universities. Revision of policies and legal frameworks for accommodating mental disabilities are only part of what is needed. As our results suggest, and as other researchers have pointed out (see Anderson, 2007), the presence of legal protection is not enough to alleviate the fear that many disabled faculty experience. Thus, we also need "proactive [policies] that generate access and connect people to each other" (Anderson, 2007, p. 185; see also Kezar et al., 2008). Achieving diversity in higher education cannot simply be hoped for; active leadership is required.
Such active leadership could include developing policies and practices that enable accommodation without requiring disclosure, in keeping with the principles of universal design (UD) (see Dolmage, 2008, 2015; Glass et al., 2013; Hamraie, 2013; Hehir, 2002; Minow, 2013). UD aims to create accessibility for the greatest range of bodyminds possible, but its concepts go beyond practical measures to include values as well. It also assumes that the way spaces are designed has much to do with the designers' beliefs about "who will (and should) inhabit the world" (Hamraie, 2013, n.p.) In other words, from a UD perspective, the design of a space ("space" here indicating social and attitudinal as well as physical features) constructs the person who is assumed to be the appropriate inhabitant of that space. In turn, inhabitants who "misfit" with this design (Garland-Thomson, 2011) will have difficulty inhabiting it, or will be absent altogether.
Of course, it's easier to call for UD in the abstract than to implement it in specific locations. As Dolmage (2008, 2015), Price (2011) and others have pointed out, the "universal" part of the UD moniker is an aspiration rather than a destination. Access requires ongoing, ever-shifting responses to the changing features of individual disabilities, local contexts, and other factors (Hamraie, 2013, 2016; Nishida, 2016). For this reason, we hesitate to offer a checklist of desirable behaviors, which might imply that the problems identified in this article are relatively easy to fix (Wood, Dolmage, Price and Lewiecki-Wilson, 2014). However, our findings do indicate that universities and colleges should prioritize clarity and transparency when attempting to improve access for faculty with mental disabilities. It should not be assumed that a single "disclosure" conversation with a single person or office will provide all accommodations needed. Moreover, faculty with mental disabilities should not be responsible for doing all the awareness-raising and education on this topic. A culture of access, emphasizing collective accountability, must be fostered (Brewer, Selfe & Yergeau, 2014; see also Nishida, 2016).8
But how, concretely, might that be done? Aimi Hamraie (2016) describes "meaningful access" as something that can be achieved only in relation: it is "learned through interaction and materialized through reciprocal encounters" (p. 266). Such interactions and reciprocal encounters unfold over time, and look different in each new iteration. An example9 comes from Mia Mingus (2010), who narrates the experience of a collective of disabled people at the Allied Media Conference as they shared responsibility for movement, food, bathing, paying for basic needs, keeping fragrance-free and maintaining shelter.
Mingus's account emphasizes that this extended moment of collective care was grounded not just in logistics, but also in feeling:
[With collective access], when I say something is inaccessible, you don't just think "there's no ramp" or "there are no places to sit" or "there's no close, accessible, free parking." Instead, you feel. You feel the weight of what inaccessibility means to us. You understand inaccessibility to mean isolation, shame, exclusion, disappointment, loneliness, anger, privilege, sadness, loss of community and disconnection. For eight days, it was amazing to be with people who know what "accessibility" means; who know and feel the weight of it; and who are working to transform it.
Mingus's (2010) point about the centrality of feeling may help explain why access, so long considered a general good in academic life, is nevertheless so often ignored or obstructed. Inhabitants of academic space are usually encouraged to think of access as a logistical problem: stairs, hallways, time limits, equipment, services (see Titchkosky, 2011). But access is also an affective problem, one that can be emotionally devastating for those barred from spaces or experiences, and one that perhaps requires feeling to push forward the collective sense of urgency and accountability that is needed to effect change.
In addition to imagining collective accountability in academic spaces, we also want to "wonder forward" (drawing upon Titchkosky's (2011) "politics of wonder") about what sort of research might be needed. Our survey, by necessity, was limited in its aims. For example, we did not attempt to measure the prevalence of mental disability among the professoriate as a whole, nor did we attempt to achieve a representative sample of respondents. Our efforts to reach out to a diverse pool of respondents, especially with respect to race, fell short; this is indicative both of our own locations as white researchers, and also of the need for Disability Studies to continue listening to and learning from scholars such as Nirmala Erevelles (2011), D. L. Adams and Nirmala Erevelles (2015), Tamika Carey (2016), and Sami Schalk (2017), who help show that critical race work surrounding disability, health, and wellness must be grounded in the work and experiences of people of color. We hope that this first large-scale survey of faculty with mental disability will lead to more investigations.
But there is much more to do. As we've talked about this survey in professional contexts, we've been asked—What about graduate students and staff? What about violence on campuses? What about comparative work between U.S. campuses and those in other countries? These are important questions. We situate the present survey as a beginning, one that we hope will serve as a basis for researchers in future investigations.
Improving access for mental disability in academia will require both idealism and practicality. While constantly reaching toward the ideal of accommodating all bodyminds, we must simultaneously acknowledge that solutions are often partial and limited, and that injustice—the simple (or not so simple) refusal of access, the abhorrence of difference, the perpetuation of violence—will continue, and must be resisted. Our ongoing efforts to construct and sustain space for faculty with mental disabilities will, we hope, be a part of radical change for all inhabitants of academic life. And life.
References
- Abram, S. (2003). The Americans with Disabilities Act in higher education: The plight of disabled faculty. Journal of Law and Education 32(1), 1-19.
- Adams, D. L. and N. Erevelles. (2015). Shadow play: DisCrit, dis/respectability and carceral logics. In D. Connor, B. Ferri and A.S. Annamma (Eds.), DisCrit: Disability studies and critical race theory in education. New York: Teachers College Press.
- American Association of University Professors. (2012). Accommodating faculty members who have disabilities. Retrieved from http://www.aaup.org/report/accommodating-faculty-members-who-have-disabilities.
- Anderson, R. (2007). Faculty members with disabilities in higher education. In M. L. Vance (Ed.), Disabled faculty and staff in a disabling society: Multiple identities in higher education (pp. 183-200). Huntersville, NC: AHEAD.
- Aubrecht, K. (2014). Disability studies and the language of mental illness. Review of Disability Studies 8(2), 31-44.
- Avinger, C., Croake, E., & Miller, J. K. (2007). Breathing underwater in academia: Teaching, leaning, and working with the challenges of invisible illnesses and hidden (dis-)abilities. In M. L. Vance (Ed.), Disabled faculty and staff in a disabling society: Multiple identities in higher education (pp. 201-215). Huntersville, NC: AHEAD.
- Baldridge, D. C. & Swift, M. L. (2013). Withholding requests for disability accommodation: The role of individual differences and disability attributes. Journal of Management 39(3), 743-762. https://doi.org/10.1177/0149206310396375
- Baldridge, D. C. & Viega, J. F. (2006). The impact of anticipated social consequences on recurring disability accommodation requests. Journal of Management 32(1), 158-179. https://doi.org/10.1177/0149206305277800
- Boyce, M., Secker, J., Johnson, R., Floyd, M., Grove, B., Schneider, J. & Slade, J. (2008). Mental health service users' experiences of returning to paid employment. Disability & Society 23(1), 77-88. https://doi.org/10.1080/09687590701725757
- Brandzel, A. L. & Desai, J. (2008). Race, violence and terror: The cultural defensibility of heteromasculine citizenship in the Virginia Tech massacre and the Don Imus affair. Journal of Asian American Studies 11(1), 61-85. https://doi.org/10.1353/jaas.2008.0005
- Brewer, E., Selfe, C. L., & Yergeau, M. (2014). Creating a culture of access in composition studies. Composition Studies 42(2), 151-54.
- Brohan, E., Henderson, C., Wheat, K., Malcolm, E., Clement, S., Barley, E., Slade, M., and Thornicroft, G. (2012). Systematic review of beliefs, behaviours and influencing factors associated with disclosure of a mental health problem in the workplace. BMC Psychiatry 12(1): 11–25. https://doi.org/10.1186/1471-244X-12-11
- Brottman, M. (2007). DSM-IV 300.30. In K.R. Myers (Ed.), Illness in the academy: A collection of pathographies by academics (pp. 347-355). West Lafayette, IN: Purdue University Press.
- Brueggemann, B. J. (1999). On (almost) passing. In B. J. Brueggemann, Lend me your ear: Rhetorical constructions of deafness (81-99). Washington, D.C.: Gallaudet University Press.
- Brune, J. A. & Wilson, D. J. (Eds.). (2013). Disability and passing: Blurring the lines of identity. Philadelphia: Temple University Press.
- Carey, T. L. (2016). Rhetorical healing: The reeducation of contemporary black womanhood. Albany, NY: SUNY Press.
- Clark, H. (2007). Invisible disorder: Passing as an academic. In K.R. Myers (Ed.), Illness in the academy: A collection of pathographies by academics (pp. 123-130). West Lafayette, IN: Purdue University Press.
- Dalgin, R. S. & Bellini, J. (2008). Invisible disability disclosure in an employment interview: Impact on employers' hiring decisions and views of employability. Rehabilitation Counseling Bulletin 52(1), 6-15. https://doi.org/10.1177/0034355207311311
- Dawkins, M. A. (2012). Clearly invisible: Racial passing and the color of cultural identity. Waco, TX: Baylor University Press.
- Dolmage, J. (2015). Universal design: Places to start. Disability Studies Quarterly 35(2). https://doi.org/10.18061/dsq.v35i2.4632
- Dolmage, J. (2008). Mapping composition: Inviting disability in the front door. In C. Lewiecki-Wilson & B. J. Brueggemann (Eds.), Disability and the teaching of writing: A critical sourcebook (pp. 14-27). Boston: Bedford/St. Martin's.
- Donaldson, E. J. (2002). The corpus of the madwoman: Toward a feminist disability studies theory of embodiment and mental illness. NWSA Journal 14(3), 99-119. https://doi.org/10.2979/NWS.2002.14.3.99
- Donaldson, E. J. (2011). Revisiting the corpus of the madwoman: Further notes toward a feminist disability studies theory of mental illness. In K.Q. Hall (Ed.), Feminist Disability Studies (pp. 91-113). Bloomington: Indiana UP.
- Emmons, K. K. (2010). Black dogs and blue words: Depression and gender in the age of self-care. New Brunswick, NJ: Rutgers University Press.
- Erevelles, N. (2011). Disability and difference in global contexts: Enabling a transformative body politic. New York: Palgrave Macmillan. https://doi.org/10.1057/9781137001184
- Faculty with disabilities survey. (2011). FORWARD Initiative, North Dakota State University. Retrieved from http://www.ndsu.edu/fileadmin/forward/documents/Faculty_with_Disabilities_Survey_March_2012.pdf
- Garland-Thomson, R. (2011). Misfits: A feminist materialist disability concept. Hypatia 26(3), 591-609. https://doi.org/10.1111/j.1527-2001.2011.01206.x
- Glass, D., Meyer, A., & Rose, D. H. (2013). Universal Design for learning and the arts. Harvard Educational Review, 83(1), 98-119. https://doi.org/10.17763/haer.83.1.33102p26478p54pw
- Goldberg, S. G., Killeen, M. B., & O'Day, B. (2005). The disclosure conundrum: How people with psychiatric disabilities navigate employment. Psychology, Public Policy and Law 11(3), 463-500. https://doi.org/10.1037/1076-8971.11.3.463
- Hamraie, A. (2013). Designing collective access: A feminist disability theory of universal design. Disability Studies Quarterly 33(4). https://doi.org/10.18061/dsq.v33i4.3871
- Hamraie, A. (2016). Beyond accommodation: Disability, feminist philosophy, and the design of everyday academic life. PhiloSOPHIA 6(2): 259-271. https://doi.org/10.1353/phi.2016.0022
- Hogan, R. (2007). The manic-depressive professor. In K.R. Myers (Ed.), Illness in the academy: A collection of pathographies by academics (pp. 131-136). West Lafayette, IN: Purdue University Press.
- Irvine, A. (2011). Something to declare? The disclosure of common mental health problems at work. Disability & Society 26(2), 179-192. https://doi.org/10.1080/09687599.2011.544058
- Hehir, T. (2002). Eliminating ableism in education. Harvard Educational Review, 72(1), 1-32. https://doi.org/10.17763/haer.72.1.03866528702g2105
- Hogan, R. (2007). The manic-depressive professor. In K.R. Myers (Ed.), Illness in the academy: A collection of pathographies by academics (pp. 131-136). West Lafayette, IN: Purdue University Press.
- Horton, J. & Tucker, F. (2014). Disabilities in academic workplaces: Experiences of human and physical geographers. Transactions of the Institute of British Geographers, 39, 76-89. https://doi.org/10.1111/tran.12009
- Jago, B. J. (2007). Coming out with my academic depression. In K. R. Myers (Ed.), Illness in the academy: A collection of pathographies by academics (pp. 110-122). West Lafayette, IN: Purdue University Press.
- Jamison, K. R. (1995). An unquiet mind: A memoir of moods and madness. New York: Random House / Vintage Books.
- Kerschbaum, S. L. (2014). On rhetorical agency and disclosing disability in academic writing. Rhetoric Review, 33(1), 55-71. https://doi.org/10.1080/07350198.2014.856730
- Kerschbaum, S. L., Garland-Thomson, R., Oswal, S. K., Vidali, A., Ghiaciuc, S., Price, M., Dolmage, J., Meyer, C. A., Brueggemann, B. J., & Samuels, E. (2013). Faculty members, accommodation, and access in higher education. Profession. Retrieved from http://profession.commons.mla.org/2013/12/09/faculty-members-accommodation-and-access-in-higher-education/
- Kerschbaum, S. L., A. M. O'Shea, M. Price, and M. Salzer. (in press). "Accommodations and disclosure for faculty members with mental disability." In S. L. Kerschbaum, L. T. Eisenman, and J. M. Jones (Eds.), Negotiating disability: Disclosure and higher education. Ann Arbor: U of Michigan P.
- Kerschbaum, S. L. and Price, M. (in press). Centering disability in qualitative interviewing. Research in the Teaching of English.
- Kezar, A., Eckel, P., Contreras-McGavin, M. & Quaye, S. J. (2008). Creating a web of support: An important leadership strategy for advancing campus diversity. Higher Education 55(1), 69-92. https://doi.org/10.1007/s10734-007-9068-2
- Laden, V.A. & Schwartz, G. (2003). Psychiatric disabilities, the Americans with Disabilities Act, and the new workplace violence account. In L. H. Krieger (Ed.), Backlash against the ADA: Reinterpreting disability rights. Ann Arbor: University of Michigan Press.
- LeFrançois, B.A., Menzies, R. & Reaume, G. (2013). Mad matters: A critical reader in Canadian Mad studies. Toronto: Canadian Scholars' Press.
- Lewiecki-Wilson, C. (2003). Rethinking rhetoric through mental disabilities. Rhetoric Review 22(2), 156-67.
- Mingus, M. (2010). Reflections on an opening: Disability justice and creating collective access in Detroit." Leaving Evidence. August 23, 2010. https://leavingevidence.wordpress.com/2010/08/23/reflections-on-an-opening-disability-justice-and-creating-collective-access-in-detroit/
- Minow, M. (2013). Universal design in education. In A. S. Kanter and B. A. Ferri (Eds.), Righting educational wrongs: Disability studies in law and education (pp. 38-57). Syracuse, NY: Syracuse University Press.
- Montgomery, C. (2001). A hard look at invisible disability. Ragged Edge Online 22(2). Retrieved from http://www.ragged-edge-mag.com/0301/0301ft1.htm.
- Mullings, B., Peake, L. & Parizeau, K. (2016). Cultivating an ethic of wellness in geography. The Canadian Geographer 60(2), 161-167. https://doi.org/10.1111/cag.12275
- Myers, K. R. (Ed.) (2007). Illness in the academy: A collection of pathographies by academics. West Lafayette, IN: Purdue University Press.
- Nishida, A. (2016). Neoliberal academia and a critique from disability studies. Occupying Disability: Critical Approaches to Community, Justice, and Decolonizing Disability. Ed. Pamela Block, Devva Kasnitz, Akemi Nishida and Nick Pollard. New York: Springer. 145-157. https://doi.org/10.1007/978-94-017-9984-3_10
- Prendergast, C. (2001). On the rhetorics of mental disability. In J. C. Wilson and C. Lewiecki-Wilson (Eds.), Embodied Rhetorics: Disability in Language and Culture (pp. 45-60). Carbondale: Southern Illinois UP.
- Price, M. (2011). Mad at school: Rhetorics of mental disability and academic life. Ann Arbor: University of Michigan Press. https://doi.org/10.3998/mpub.1612837
- Price, M. (in press). The precarity of disability/studies in academe. In W.S. Hesford, A.C. Licona and Christa Teston (Eds.), Precarious Rhetorics. Columbus, OH: The OSU Press.
- Price, M. (2017). Un/shared space: The dilemma of inclusive architecture. In J. Boys (Ed.), Disability, space, architecture: A reader (pp. 155-172). New York/London: Routledge.
- Price, M. and S. L. Kerschbaum. (2016). Stories of methodology: Interviewing sideways, crooked and crip. Canadian Journal of Disability Studies 5(3). https://doi.org/10.15353/cjds.v5i3.295
- Pryal, K. R. G. (2014, June 13). Disclosure blues: Should you tell colleagues about your mental illness? Vitae. The Chronicle of Higher Education. Retrieved from https://chroniclevitae.com/news/546-disclosure-blues-should-you-tell-colleagues-about-your-mental-illness
- Railton, P. (2015). Innocent abroad: Rupture, liberation and solidarity. American Philosophical Society. Retrieved from http://dailynous.com/2015/02/22/peter-railtons-dewey-lecture/.
- Reaume, G. (2002). Lunatic to patient to person: Nomenclature in psychiatric history and the influence of patients' activism in North America. International Journal of Law and Psychiatry 25, 405-426. https://doi.org/10.1016/S0160-2527(02)00130-9
- Saks, E. R. (2007). The center cannot hold: My journey through madness. New York: Hyperion.
- Salzer, M. S. (2012). A comparative study of campus experiences of college students with mental illnesses versus a general college sample. Journal of American College Health, 60(1), 1-7. https://doi.org/10.1080/07448481.2011.552537
- Salzer, M. S., Wick, L. C. & Rogers, J. A. (2008). Familiarity with and use of accommodations and supports among postsecondary students with mental illnesses. Psychiatric Services, 59(4), 370-375. https://doi.org/10.1176/ps.2008.59.4.370
- Samuels, E. (2003). My body, my closet: Invisible disability and the limits of coming-out discourse. GLQ, 9(1), 233-255. https://doi.org/10.1215/10642684-9-1-2-233
- Samuels, E. (2007). Panic. In K.R. Myers (Ed.), Illness in the academy: A collection of pathographies by academics (pp. 330-335). West Lafayette, IN: Purdue University Press.
- Schalk, Sami. (2017). Critical disability studies as methodology. Lateral 6.1 (Spring 2017). http://csalateral.org/issue/6-1/forum-alt-humanities-critical-disability-studies-methodology-schalk/
- Shigaki, C. L., Anderson, K. M., Howald, C. L., Henson, L., & Gregg, B. E. (2012). Disability on campus: A perspective from faculty and staff. Work 42(4): 559-71.
- Siebers, T. (2004). Disability as masquerade. Literature and Medicine, 23(1), 1-22. https://doi.org/10.1353/lm.2004.0010
- Siebers, T. (2008). Disability theory. Ann Arbor: University of Michigan Press. https://doi.org/10.3998/mpub.309723
- Skogen, R. (2012). 'Coming into presence' as mentally ill in academia: A new logic of emancipation. Harvard Educational Review, 82(4), 491-510. https://doi.org/10.17763/haer.82.4.u1m8g0052212pjh8
- Smith, D. H. & Andrews, J. F. (2015). 'Deaf and hard of hearing faculty in higher education: Enhancing access, equity, policy and practice.' Disability & Society 30(10), 1521-1536. https://doi.org/10.1080/09687599.2015.1113160
- Snitker, M. (2007). Among the ranks of faculty. In M.L. Vance (Ed.), Disabled faculty and staff in a disabling society: Multiple identities in higher education (pp. 147-153). Huntersville, NC: AHEAD.
- Thomas, K. (2014, May 8). We don't want anyone to know, say depressed academics. The Guardian. Retrieved from http://www.theguardian.com/higher-education-network/blog/2014/may/08/academics-mental-health-suffering-silence-guardian-survey
- Titchkosky, T. (2011). The question of access: Disability, space, meaning. Toronto: University of Toronto Press.
- Tsipursky, G. (2015, May 8). Teaching while anxious: The challenges of teaching with a mental health condition. Inside Higher Education. Retrieved from https://www.insidehighered.com/advice/2015/05/08/challenges-teaching-mental-health-condition-essay.
- Vance, M. L. (Ed.) Disabled faculty and staff in a disabling society: Multiple identities in higher education. Huntersville, NC: AHEAD.
- Venville, A., Street, A. & Fossey, E. (2014). Student perspectives on disclosure of mental illness in post-compulsory education: Displacing doxa. Disability & Society 29(5): 792-806. https://doi.org/10.1080/09687599.2013.844101
- Watts, I. E. & Erevelles, N. (2004). These deadly times: Reconceptualizing school violence by using critical race theory and disability studies. American Educational Research Journal 41(2), 271-299. https://doi.org/10.3102/00028312041002271
- White, R. (2007). Instructor disclosure of mental illness in the social work classroom. Social Work Forum 40/41, 127-142.
- Wood, T. (in press). "Rhetorical disclosures: The stakes of disability identity in higher education." In S. L. Kerschbaum, L. T. Eisenman, and J. M. Jones (Eds.), Negotiating disability: Disclosure and higher education. Ann Arbor: U of Michigan P.
- Wood, T., Dolmage, J., Price, M. & Lewiecki-Wilson, C. (2014). Moving beyond disability 2.0 in composition studies. Composition Studies 42(2), 147-150.
Endnotes
-
The contents of this publication were developed under a grant from the U.S. Department of Health and Human Services, National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR). Grant H133B100037 (Salzer, Principal Investigator). However, those contents do not necessarily represent the policy of the U.S. Department of Health and Human Services, and endorsement by the federal government should not be assumed.
Return to Text -
The language applied to mental health conditions varies widely (see Price, 2011; Reaume, 2002). For example, some may use mental illness on the grounds that an illness can be treated and cured, while others take a more critical view (Aubrecht, 2014; Donaldson, 2002, 2011; Irvine, 2011). A variety of other terms, including psychiatric disability, neurodiversity, madness, or mental health services user, are in use, with authors sometimes making clear distinctions along diagnostic lines and sometimes not—often for political reasons. The attempt to define a mental-health condition "is rarely a straightforward or singular process" (Emmons, 2010, p. 71). For the purposes of this article, and following the examples of Lewiecki-Wilson (2003), Prendergast (2001), and Price (2011), we use mental disability.
Return to Text -
Specifically, we informed potential participants that they qualified for the survey if they had received mental health care and/or a mental health diagnosis. For further details, see the section "Methods."
Return to Text -
This review of research does not include studies of people with mental-health disabilities navigating the workplace in general (as opposed to faculty in particular). General workplace studies include Laden & Schwartz (2003); Goldberg, Killeen & O'Day (2005); Boyce et al. (2008); Dalgin & Bellini (2008); and Irvine (2011).
Return to Text -
The full text of the survey is available upon request; please contact Margaret Price.
Return to Text -
Participants were given the option of volunteering, in a separate space, for an interview study of disabled faculty subsequently conducted by Margaret Price and Stephanie Kerschbaum. The interview study is ongoing; preliminary findings and discussion of methodology can be found in Price and Kerschbaum (2016), Price (2017), Kerschbaum and Price (in press), and Price (in press).
Return to Text -
These assertions apply to respondents to the present survey and may not be generalizable to the total population of U.S. faculty with mental disabilities. No survey or other research instrument has, to our knowledge, sampled a representative group of faculty with mental disabilities.
Return to Text -
Our survey has also led to the creation of a resource guide which presents findings in a form that can easily be taken up in on-campus initiatives. This guide, Promoting Supportive Academic Environments for Faculty with Mental Illnesses: Resource Guide and Suggestions for Practice, can be downloaded for free from the website of the Temple University Collaborative on Community Inclusion (http://tucollaborative.org/community-inclusion/resources/employment-resources/).
Return to Text -
Other examples can be found on the "Composing Access" website (https://u.osu.edu/composingaccess), which offers a variety of videos and documents to both demonstrate and explain the ways that access might unfold in specific locations; and in Hamraie's (2016) article, which describes a panel that sought to provide meaningful access through a variety of efforts, responses, and revisions.
Return to Text
