
The present research aimed to perform data survey and analysis of children and teenagers among 0- to 19-year-olds related to SARS (severe acute respiratory syndrome) and COVID-19 in populations with or without disabilities during the year of 2020. The database used for the evaluations was Sivep-Gripe, made available by the Ministry of Health. The database did not present variables regarding the type of disability and a proxy was created by the binary variable of Down syndrome and by qualitative analysis of clinical data of descriptive morbidity. This limitation hindered the consideration of the experience of disability as an interaction between bodily impairments and the environment, as well as the generalization regarding cases in this population. The analysis variables included individual, regional and progression characteristics of the cases, such as the need for hospitalization, admission to the ICU, use of ventilatory supports and evolution of the cases for the recovery or death. 83,491 cases of children up to 19 years old were considered. Of this total, 2,370 (3.27%) were categorized with the disability proxy. The analyzes showed the differences between cases and progressions between children and young people without disabilities and by type of disability, with the highest proportions of COVID-19 cases found in those with physical, intellectual or psychosocial disabilities. Considering the age groups, we found higher frequencies of these cases among children up to 4 years old in general; with intellectual or psychosocial disabilities between 5 and 9 years; and those with physical disabilities between 14 and 19 years. The progression of the children's cases demonstrates the relevance of considering their vulnerability and its effects on hospital establishments, since they are more susceptible to being hospitalized, requiring ICU admissions and respiratory support. Even with the use of these resources for the maintenance of life, the proportion of children with disabilities who evolve to death is equivalent to more than double (in the cases of COVID-19) and triple (SARS) of those without disabilities. Based on these verifications, we emphasize the need to further investigate, plan and execute public policies that target this population, especially in relation to health services in the current context of increasing cases of COVID-19 and its variants across the country. In addition, we seek to contribute to academic discussions that address disability as a relevant social marker that permeates the different layers of inequality and social exclusion, exposed and deepened in the pandemic context.
Introduction
In Brazil, according to the 2010 census 1, 6,7% of the population has some type of disability. 2 Among children and adolescents up to 19 years old, 2.88% have disabilities, the highest number of those being persons with intellectual disabilities among residents of the North and Northeast regions of the country. These regions have the highest indices of social vulnerability (Gini Index) and this inequality is related to higher rates of infection and mortality from COVID-19 in children and adolescents up to 19 years of age, as verified by Martins-Filho et al (2021). The authors emphasize that although the evidence accumulated so far has shown that the mortality of children from COVID-19 is extremely rare in developed countries, in Brazil the disease has been a significant cause of death of children in poorer communities and in more vulnerable regions, evidencing the close relationship between the incidence of cases and socioeconomic inequalities.
Besides being in the most unequal regions, according to the 2010 census, children and adolescents with disabilities have less access to education and literacy: between 5 and 9 years old, while 6% of those without disabilities are literate, only 0.44% of those with disabilities are. Between the ages of 10 and 19, these rates are 9% and only 1%, respectively. The lower level of education of persons with disabilities is also found considering other age groups, since the rates of persons who have a higher level of education is half of that found in the population without disabilities. Regarding socioeconomic inequalities, we note that in households with a resident with disabilities, incomes are lower than those without residents with disabilities; and that persons with disabilities in Brazil are the poorest of the poor: even receiving of the Continuous Cash Benefit provided by the Organic Law of Social Assistance - LOAS 3 (Brasil, 1993), they remain in the lowest range of per capita income, corresponding to a quarter of a minimum wage (Almeida, 2019). In this light, when considering the context of a pandemic, it is clear how disability is politically engendered from the intersection of social markers which place these persons in greater vulnerability (Schuch & Sarreta, 2020).
However, as highlighted by Fietz et al (2020), for general policies of prevention and mitigation of the pandemic to be truly effective, they must take into account the singularities of the bodies and the social and cultural contexts in which they occur. Some experiences cannot not be excluded a priori from global health policies that should actually protect them. Particularly for persons with disabilities who depend on others for daily activities, the physical proximity of caregiving relationships is indispensable to their survival and a complicating factor to the observance of recommendations. On the other hand, all the work done by their network of support and care, which is most of the time invisible, is a threat of contagion exacerbated by the conditions of poverty in which most persons in Brazil find themselves (Fietz et al., 2020).
The debate about care policies for persons with disabilities is of special concern when considering the effects of the COVID-19 pandemic on children and adolescents with disabilities. According to the 2013 National Health Survey (PNS) 4 regarding age and other factors that lead to disability, a minority of persons in Brazil are born with some disability, the vast majority of cases being acquired in the course of a lifetime. The rise in children and adolescents with disabilities with age can be observed in Brazil through the 2010 census data. Between 0 and 4 years old, only 0.2% of children have some kind of disability; between 5 and 9 years old, 0.6%; and between 10 and 19 years old, this rate doubles among adolescents. Intellectual disability is more prevalent and its rates increase with age - from 0.03 (0-4 years) to 0.10% (14-19 years).
In this respect, Sen (2009) notes that only a fairly moderate proportion of persons living with disability had their condition determined during pregnancy or even during birth; it is easily observable how poverty can increase the chances of acquiring a disability through different ways - most of them related to poor health and its determinants. In developing countries, there is evidence of a link between maternal malnutrition in infancy and disability. Another way would be through diseases that have prevalence and incidence strongly associated with poverty due to lack of public health interventions (immunization), poor housing conditions (such as lack of clean water), and increased exposure to environmental (lack of safe working conditions) and accidental hazards (Mitra et al., 2013; Sen, 2009).
In Brazil, regarding the disability-poverty interface, we highlight the researches developed by Anis 5 – Bioethics Institute, especially in relation to the project about Zika virus, women and rights, in which they verified that the epidemic of this virus mirrors the inequality of Brazilian society. In the study conducted by Diniz (2017), the mothers of children affected by the epidemic are mostly adolescents or very young, black and indigenous, with poor education, unemployed, and completely dependent on welfare policies. Those who quit their jobs to care for the children reported the negative and immediate effects it had on the household economy.
Even when receiving the Continuous Cash Benefit, Diniz (2017) points out that women became full-time caregivers, since the income from the benefit is entirely dependent on the woman's permanence in the home as a caregiver. As the beneficiary is the child and not the mother for her work, there would be "a disappearance of the female caregiver with rights or needs, and the emergence of a figure of excessive mothering - either for child care or for family survival". In that way, as a caregiver, the woman's role as a citizen is not considered in social policies of income transfer or for contributory retirement policies. "Moreover, for a return to paid work, her years as a caregiver will have permanent exclusionary effects, especially if added to the poor education of the vast majority of women" (Diniz, 2017: 45, our translation).
Regarding access to clean drinking water and sanitation in households, we observe that in Brazil, according to the 2010 census, persons with disabilities have less access than those without disabilities. The lack of these services in households is mainly observable among persons with physical and intellectual disabilities (Almeida, 2019). This deprivation is relevant to the condition of poverty experienced by much of this population, as well as a possible cause of disability and morbidities, since the lack of these resources in the home can have implications for family dynamics and a greater chance of persons with disabilities, notably those with great physical/motor difficulty, to acquire diseases (Alam & Bryant, 2016; Groce et al., 2011; Groce, 2009).
On this matter, we stress that the Convention on the Rights of Persons with Disabilities, ratified in Brazil by Decree nº 6,949/2009 (Brasil, 2009) ensures equal access of persons with disabilities to basic sanitation services, and Law nº 13,146/2015 - Brazilian Inclusion Law (Brasil, 2015) seeks to promote, at the federal level and in conjunction with the States, the Federal District, and the Municipalities, programs to build housing and improve housing conditions, basic sanitation, sidewalks, and walkways. However, what we find in almost all the states is that persons with disabilities have less access to basic sanitation. Furthermore, the debate about the need for access to basic sanitation is particularly relevant in the face of the COVID-19 epidemic, considered the forms of infection (Lodder & Husman, 2020).
Research regarding factors that go beyond income and consider the different deprivations that can lead to a multidimensional poverty condition, such as individual and household characteristics, access to goods and services, as proposed by Amartya Sen (2009) in the capabilities approach, and that used the method proposed by Alkire and Foster (2011a, 2011b) indicate that persons with disabilities are in this poverty condition in higher rates than those without disabilities in different developing countries, including Brazil (Almeida, 2019; Mitra et al., 2013; Mitra & Sambamoorthi, 2008; Mizunoya & Mitra, 2013; Mizunoya et al., 2018; Trani et al., 2018; Trani & Loeb, 2012).
In this direction, Mitra (Mitra, 2006) suggests Amartya Sen's capabilities approach for understanding poverty as a contributing factor that interacts with the individual's characteristics and environment and may lead to disability. Based on this approach, on the World Health Organization's International Classification of Functioning, Disability and Health - ICF - and on discussions about the medical and social models of disability, the author proposes the human development model of disability (Mitra, 2017), contemplating in its structure the growing evidence of socioeconomic determinants of health developed by the field of social epidemiology.
In order to understand disability, Mitra (2017) suggests that the capability approach allows it to be differentiated on two levels: on the capability level (as potential disability), and on the functioning level (as actual disability), since there is great diversity in the connection and relationships between a given bodily impairment and the resulting disability which depends on the interaction of different factors: impairments, individual characteristics, resources, and the environment (structural factors). The dynamics among these factors are continuous, multidimensional, and result in a potentially heterogeneous notion of well-being and disability. Therefore, bodily impairments are necessary but not sufficient components for disability.
Factors related to individual characteristics can comprise simple demographic information (such as sex, race/ethnicity, and age). Resources include access to goods, income, services, and information, and may belong to the individual or be resources that can be accessed through family or community (public goods). Structural factors, on the other hand, are broad and cover physical, social, economic, epidemiological, and political aspects of the individual's context - they refer to the characteristics of his or her environment, whether the immediate environment (e.g., family, home, and workplace), the meso-environment (the community), and the macro-environment (regional, national). At each of these levels, structural factors can influence capabilities and functionalities.
From this definition, not all persons with bodily impairments or health restrictions necessarily have a disability, but all have some potential to have one (Mitra, 2017), given that disability is defined as a deprivation in terms of functionality and/or capability among persons with bodily impairments, resulting from the interaction between these impairments and individual characteristics, available socioeconomic resources, and structural factors. In this light, the consideration of these factors and their interactions to the experience of disability enables the design and implementation of public policies aimed at improving the living conditions and well-being of the population with disabilities (Mitra, 2017). We argue that in the human development model the focus is to verify how bodily impairments can relate to other dimensions of well-being. The purpose of research or policy initiatives guided by this model is to improve human development, i.e., to expand the functionality/capabilities of individuals in health deprivation or to expand functionality/capabilities while avoiding health deprivation. Resources or structural factors (health services, care mechanisms) and other means may be used to achieve this goal, but are not ends in themselves (Mitra, 2017).
On this point, we stress that Nussbaum (2013), regarding Sen's capability approach, adds that all citizens are entitled, based on social justice, to all capabilities, up to an adequate minimum level. If persons are below that minimum level in any of the capabilities, that is a failure of basic justice, no matter how advanced they are in all the others. Thus, what is wrong with using income and wealth as measures of social position cannot be fully captured by insisting on variability in the need for resources: the problem already lies in treating capabilities as fungible according to a single measure.
According to Nussbaum (2013), a clear flaw in the current legal situation regarding the care of persons with disabilities is that the work of women in the family is not recognized as such. The author highlights Eva Kittay's (1999) suggestion that the best way to remedy this situation would be direct payment to all family members who perform care work, and points out that thinking carefully about care implies broad consideration of capabilities on both the side of those who care and those who are cared for. Thus, good care for the dependent (children, the elderly, or persons with disabilities) has at its core the support of capabilities in the realm of life, health, and integrity (Nussbaum, 2013).
Therefore, we consider that the approach to disability through the human development model is relevant to the understanding of the experience of disability in the face of a pandemic, since it considers it in a continuous and dynamic way as a result of interactions between structural, socioeconomic, individual factors and bodily impairments. The mapping of these factors and the way they are articulated enables the development of public policies that consider bodily diversity and focus on access to public goods and services that are crucial in the current context of full expansion of the COVID-19 epidemic in Brazil, since this population already finds itself in a situation of social vulnerability, as presented by data from the 2010 census. Nussbaum's (2013) considerations expand the need for public policies' focus to go beyond persons with disabilities, especially considering the work of female caregivers, which is not recognized as such. This discussion is especially relevant when taking into account infants, children and adolescents with disabilities.
In this article we seek to present the national data regarding children and adolescents with disabilities, aged 0-19 years, in relation to cases of infection and death from COVID-19 and SARS (severe acute respiratory syndrome). In a previous study in Brazil regarding this population and infection and mortality rates, COVID-19 has been found to be a relevant cause of death in the poorest communities and most vulnerable regions (Martins-Filho et al., 2021), although not addressing disability.
However, in Brazil, administrative and demographic data and surveys that have disability-related variables are scarce. The database of the Ministry of Health, which is filled with information about individuals who may have COVID-19, has serious limitations that prevent consideration of the actual number of persons with disabilities infected, as well as a large under-notification (because it only considers confirmed cases) and delays in the reporting of cases. Given this large gap of data regarding COVID-19 and children and adolescents with disabilities, we aimed to collect and analyze, albeit incipiently, cases and deaths by age group and variables related to their region and individual characteristics, and other variables related to the progression of cases, such as hospitalization, admission to Intensive Care Units (ICU), use of ventilatory support, and evolution of cases, in order to foster the study and planning of public policies focused on improving the welfare of this population.
To this end, in addition to this introduction, we present the employed methodology, the data analysis, and the final considerations.
Methodology
Although most developing countries do not have an integrated national system to identify the individual characteristics of patients and the receiving hospitals in order to assess impacts on the health system (Ranzani et al., 2021), Brazil performs this monitoring through the unified health information system - DATASUS. The information collected by this system is made available in databases by the Ministry of Health (MS), which, through the Secretariat of Health Surveillance (SVS), performs surveillance of severe acute respiratory syndrome (SARS) in Brazil since the Influenza A(H1N1) pandemic in 2009. In 2020, surveillance of COVID-19, a human infection caused by the new Coronavirus, was incorporated into the surveillance network for Influenza and other respiratory viruses.
The epidemiological databases of SARS, from the surveillance network of Influenza and other respiratory viruses are made available grouped with updates of the surveillance of COVID-19 on the website of the Ministry of Health. 6 Currently, the official system for recording cases and deaths from SARS is the Influenza Epidemiological Surveillance Information System (SIVEP-Gripe). For this study, we used the database made available on June 14, 2021, since it was the most recent at the time of this research and allowed the presentation of the evolution of the number of cases during the previous year. However, we emphasize that these results present a large under-reporting, as they only register severe and confirmed cases.
In this regard, we selected SARS (severe acute respiratory syndrome) and COVID-19 cases related to the population of children and adolescents aged 0 to 19 years. These cases were considered from the variable referring to the final classification of the case, where we regarded unspecified SARS and SARS as COVID-19. 7 The variables and categories selected for analysis were:
- month of case notification: months of the year 2020;
- age: from 0 to 19 years aggregated in age groups: 0 to 4 years, 5 to 9 years, 10 to 14 years, 15 to 19 years;
- color/race: white, black, pardo, yellow, and indigenous;
- sex: male and female;
- region of case notification: North, Northeast, Central-west, Southeast, South;
- Down's Syndrome: yes or no;
- has risk factors: yes or no:
- hospital admission: yes or no;
- admission to Intensive Care Unit (ICU): yes or no;
- use of ventilatory support: yes or no, invasive or non-invasive;
- evolution of the case: cure, death or death from other causes.
To consider disability, we took into account all cases in which there was an indication that the patient had Down's Syndrome, which was added to the Sivep-Gripe database during the year 2020, and in addition, to contemplate other types of disability, it was necessary to make an approximation from the descriptive data entered in the descriptive morbidity variable. The analysis carried out with this field was necessary since the Ministry of Health's Sivep-Gripe micro data bank does not include a variable on whether or not a person has a disability. 8 Thus, to create the proxy variable for disability, we considered the indication of the Chromosome XXI syndrome and the morbidities described by the health team professionals in the field referring to the descriptive morbidity.
The data analysis of the described terms entered by the health teams was performed considering all the terms entered for the individuals in the study population, which led us to a total of 2200 morbidity descriptions. The qualitative analysis was performed taking into account the description of the impairment and whether or not it could imply a disability. Thus, we stress that our variable of analysis represents only an approximation, since the available data refer mostly to the description of clinically indicated risk factors for COVID-19.
In this regard, it was not possible to include, in relation to most cases, the person with disability as it is conceived in Brazil since the International Convention on the Rights of Persons with Disabilities, ratified by Decree No. 6.949/2009 (Brasil, 2009), as those who have long-term physical, mental, intellectual or sensory impairments, which, in interaction with various barriers, may obstruct their full and effective participation in society on equal terms with others. This obstacle is due both to the lack of a categorical variable on disability that considers the ICF - International Classification of Functioning - and to the description of only these bodily impairments in the descriptive variable analyzed.
In our analysis, we identified the bodily impairments corresponding to those included in Decree nº 5.296/2004 (Brasil, 2004), which describes the clinical categories of impairments related to the types of disability, namely: physical disability, hearing impairment, visual impairment, and mental disability, and others included after Decree nº 6.949/2009 (Brasil, 2009), which also considers as disabilities the global development disorders and psychosocial disability.
Regarding the descriptions considered as proxy for disability, the frequency of terms referring to cerebral palsy, trisomy of the XXI chromosome (even with the specific binary variable about it), sequelae of microcephaly caused by the Zika virus infection, hydrocephalus, autism, schizophrenia, and epilepsy were considerable. Several other descriptions, but with lower frequencies, composed the analysis in which we considered these terms according to the following categories: physical disability, hearing disability, visual disability, intellectual/psychosocial disability, and multiple disabilities.
Thus, we found a total of 2,730 children and teenagers with impairments that may result in a disability. Of this total, 804 (38.62%) have Chromosome XXI syndrome (indicated in the corresponding binary variable) and 1,250 were categorized by type of disability based on the qualitative analysis. We emphasize that despite our effort to bring data and analysis regarding children and adolescents with disabilities in relation to cases of SARS and COVID-19, these analyses are not generalizable for all persons with disabilities who may have been infected in Brazil, since there is no mandatory registration of disability in the database of the Ministry of Health, as recommended by the International Convention on the Rights of Persons with Disabilities with the necessary use of the ICF as a criterion for classifying disability.
Data analysis
In the analyzed cases, notified during the year 2020 and entered in the Sivep-Gripe database on June 14, 2021, we found a total of 83,491 children and adolescents up to 19 years old. From this total, 2,370 (3.27%) were categorized with the disability proxy and in relation to sex we noticed a similar distribution, where 54% of children with or without disabilities were male. Regarding color/race, we observed higher proportions between whites and pardos, the former being prevalent among those with disabilities (44%), and pardos among children without disabilities (45%). The percentage of black and indigenous people was 4% and 0.73% among persons without disabilities, and 3% and 0.68% among those with disabilities, respectively.
As for the region of case notification, approximately 50% of SARS cases were in the Southeast region, followed by 20% in the Northeast region, for both children with and without disabilities. The COVID-19 cases presented a more balanced distribution between these two regions: 30% of the cases in the Northeast; 40% and 33% in the Southeast, both for persons with and without disabilities. We stress that due to the low number of cases considered as proxy for disability among children and adolescents with disabilities it was not possible to perform the analyses regarding the population rates of infection and mortality and compare them to the results previously found by Martins-Filho et al (2021) regarding the regions of the country for the population up to 19 years old.
| SARS | COVID-19 | |||
|---|---|---|---|---|
| Persons without disabilities | Persons with disabilities | Persons without disabilities | Persons with disabilities | |
| Region | ||||
| North | 5.56 | 4.04 | 19.28 | 9.86 |
| Northeast | 22.44 | 19.43 | 28.01 | 29.98 |
| Center-West | 6.58 | 7.94 | 12.17 | 7.89 |
| Southeast | 53.23 | 48.81 | 33.56 | 39.64 |
| South | 12.20 | 19.78 | 6.98 | 12.62 |
| Total (n) | 53651 | 1894 | 13878 | 482 |
| % | 100 | 100 | 100 | 100 |
Source: Ministry of Health - SIVEP-Gripe data – June 14, 2021.
Regarding the final classification of cases, we also observed similar proportions between the groups, with 80% referring to SARS and 20% to COVID-19. When comparing the distribution of these cases by sex and age group, it was observed in relation to SARS that 47% and 44% of the cases occurred in children up to 4 years old, and 75% and 60% up to 9 years old, among those without and with disabilities, respectively. The cases of COVID-19 are also particularly concentrated in these age groups, where we found 60% of children without and with disabilities. However, unlike the SARS cases, a quarter of the cases of COVID-19 cases occurred in adolescents between 15 and 19 years old. When considering sex in this age group and also the COVID-19 cases, we observed more cases among female adolescents among those without disabilities, and on the other hand, male adolescents among those with disabilities.
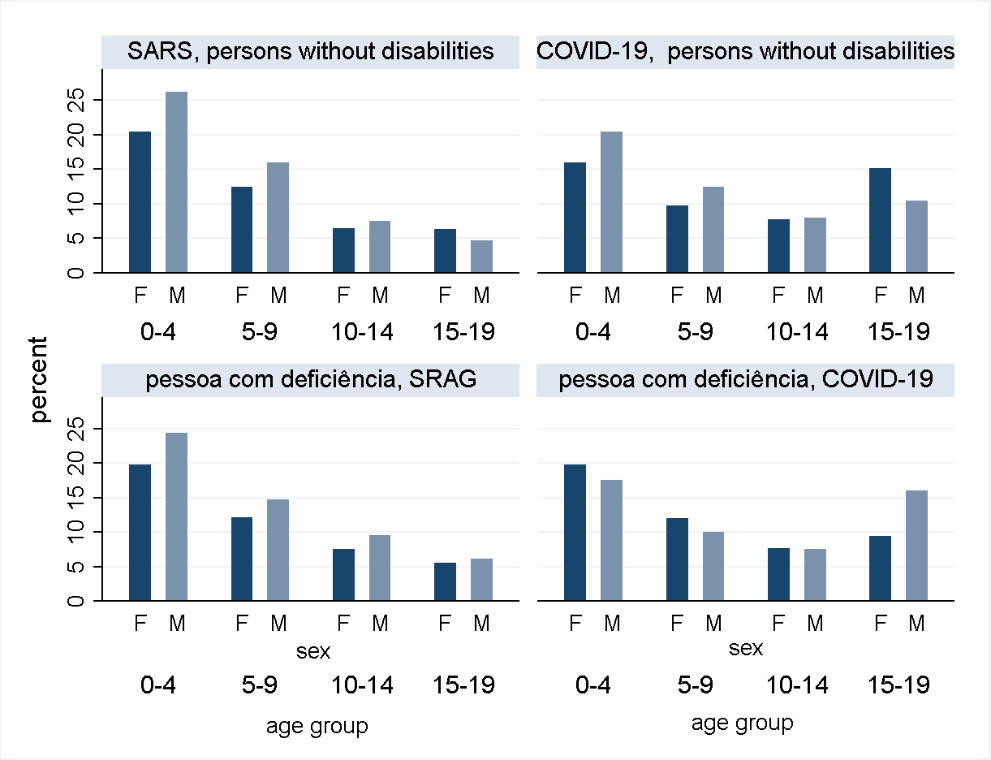
Figure 1: Percentage of SARS and COVID-19 cases by age group and sex (female, male)
Source: Ministry of Health - SIVEP-Gripe data – June 14, 2021.
Considering the SARS and COVID-19 cases by type of disability, we note the higher number of children with physical or intellectual/psychosocial disabilities, 48 and 44%, respectively, with these proportions being similar in both groups of cases. It is noteworthy, considering the age groups, the large number of cases in children up to 4 years old: 44% of the SARS cases among those with physical, intellectual, and multiple disabilities (slightly lower than that found in the total) and 46.67% of children without disabilities. Among the COVID-19 cases, we also note considerable percentages of children up to 4 years old among those without disabilities (35%), with physical disabilities (39%), or with intellectual/psychosocial disabilities (34%). However, 44% of children with multiple disabilities up to 4 years old among the COVID-19 cases are eye-catching, being 8 percentage points higher than that found in the total.
Among children aged 5 to 9 years, we noticed SARS proportions generally higher than 25% among those with and without disabilities, the lowest proportion being among those with physical disabilities. As for COVID-19, this percentage is maintained only for children with intellectual disability in this age group, and the others present a reduction to 20%.
When considering the 10 to 19 age group, we observe that between 10 and 14 years, children with disabilities present higher proportions than those without disabilities in cases of SARS, which is reversed in relation to COVID-19, with the exception of children with multiple disabilities. On the other hand, between 15 and 19 years, despite the lower proportions of SARS cases, in this age group COVID-19 cases correspond to approximately a quarter of children without disabilities, with physical and intellectual/psychosocial disabilities.
| SARS | COVID-19 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age group | Age group | |||||||||
| Type of disability | 0 to 4 years | 5 to 9 | 10 to 14 | 15 to 19 | Total | 0 to 4 years | 5 to 9 | 10 to 14 | 15 to 19 | Total |
| Without disability | 46.67 | 28.39 | 13.98 | 10.97 | 100 | 36.48 | 22.24 | 15.77 | 25.51 | 100 |
| Physical disability | 43.94 | 24.92 | 17.60 | 14.14 | 100 | 38.78 | 19.59 | 14.29 | 27.35 | 100 |
| Hearing disability | 25 | 50 | 25 | 0 | 100 | |||||
| Intellectual/psychosocial disability | 45.18 | 28.35 | 16.50 | 9.97 | 100 | 34.51 | 25.22 | 15.49 | 24.78 | 100 |
| Multiple disabilities | 44.17 | 28.83 | 19.02 | 7.98 | 100 | 44.44 | 19.44 | 19.44 | 16.67 | 100 |
| Total (n) | 28539 | 17358 | 8629 | 6739 | 61265 | 5674 | 3455 | 2448 | 3964 | 14360 |
| % | 46.58 | 28.33 | 14.08 | 14.00 | 100 | 36.51 | 22.23 | 15.75 | 25.51 | 100 |
Source: Ministry of Health - SIVEP-Gripe data – June 14, 2021.
Regarding the evolution in the number of cases over the course of 2020 9, we observed a considerable increase in the number of COVID-19 cases among children and adolescents without disabilities from May to July. When considering persons with disabilities, we observed, despite the same increase seen in the previous group, a greater stability in the number of notifications of COVID-19 cases during the last quarter, as shown in the figure below.
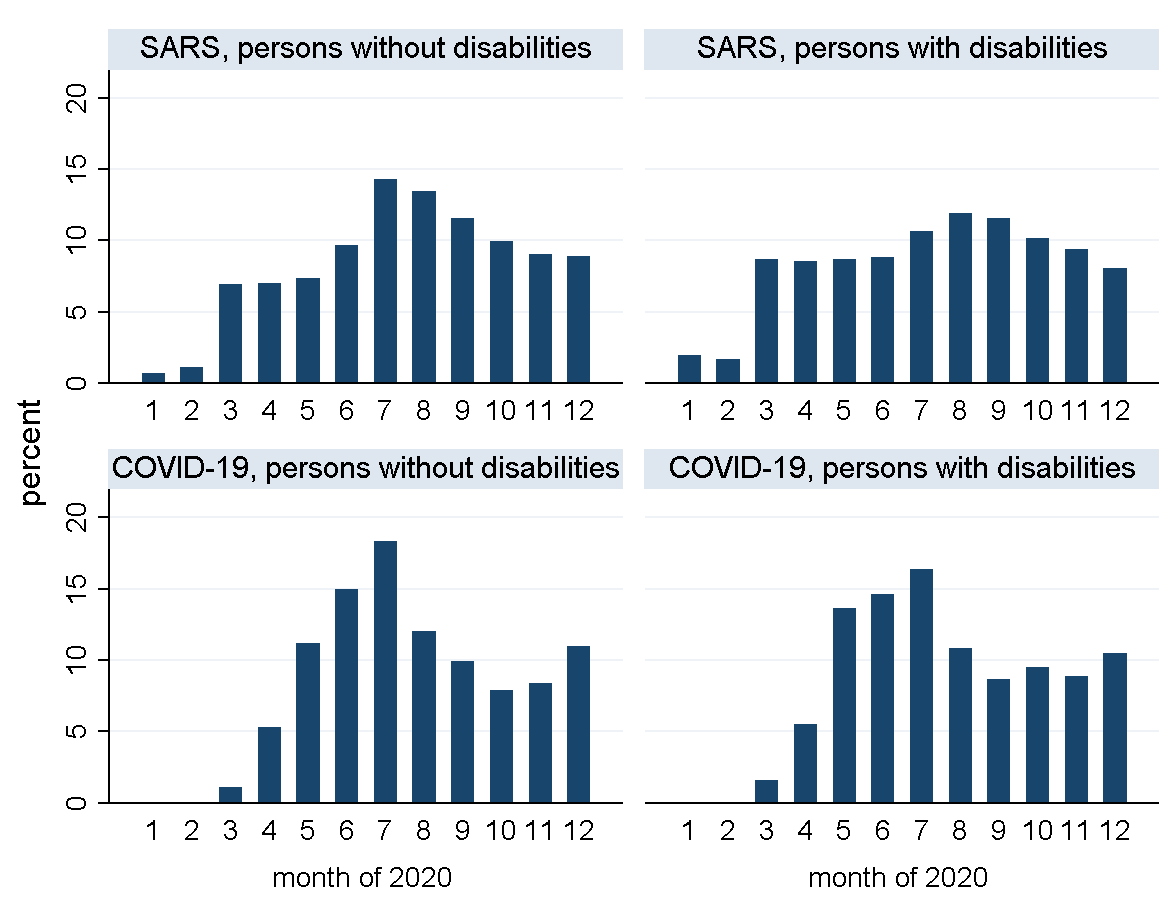
Figure 2: Evolution of SARS and COVID-19 cases - persons with and without disabilities - months of 2020
Source: Ministry of Health - SIVEP-Gripe data – June 14, 2021.
With respect to related risk factors, while most children and adolescents without disabilities do not have any, it is noticeable that all those with disabilities have some of these factors (heart disease, chronic liver disease, asthma, diabetes, pneumopathy, obesity, and others). Regarding the progression of cases of COVID-19, we note that in general, more than 90% lead to hospitalization, with the greatest difference found between persons with and without disabilities: 97% and 91%.
Once hospitalized, children and adolescents with disabilities progress more towards conditions requiring admission to Intensive Care Units (ICU): 40% in cases of SARS and 50% in cases of COVID-19. These proportions are 24% and 27% for those without and with disabilities, respectively. This scenario is similar to that found when considering the use of ventilatory support, where for up to 50% of persons without disabilities there is the use of invasive and non-invasive support, and, on the other hand, this proportion rises to 67% among patients with disabilities.
Regarding the final evolution of the hospitalized cases, we observed that more than 90% of the persons without disabilities were cured of SARS and COVID-19. This percentage drops to 77% in the case of children and adolescents with COVID-19, who present the highest percentage of deaths among the considered groups: 21%; more than double for those without disabilities. In SARS cases, the proportion of children and adolescents with disabilities who die is three times the proportion of those without disabilities: 9% and 3%.
| SARS | COVID-19 | ||||
|---|---|---|---|---|---|
| Persons without disabilities | Persons with disabilities | Persons without disabilities | Persons with disabilities | ||
| Has any risk factor | Yes | 35.31 | 100 | 31.07 | 100 |
| No | 64.69 | - | 68.93 | - | |
| Total (n) | 59212 | 2053 | 15034 | 507 | |
| % | 100 | 100 | 100 | 100 | |
| Hospitalization | Yes | 97.85 | 98.29 | 91.41 | 97.60 |
| No | 2.15 | 1.71 | 7.59 | 2.40 | |
| Total (n) | 58370 | 2042 | 14426 | 500 | |
| % | 100 | 100 | 100 | 100 | |
| ICU* | Yes | 24,69 | 40.38 | 27.07 | 48.91 |
| No | 75.31 | 59.62 | 72.93 | 51.09 | |
| Total (n) | 51807 | 1897 | 11892 | 460 | |
| % | 100 | 100 | 100 | 100 | |
| Ventilatory support* | Yes. invasive | 9.18 | 21.55 | 11.21 | 27.13 |
| Yes. non-invasive | 41.66 | 44.95 | 34.99 | 40.92 | |
| No | 49.16 | 33.50 | 53.80 | 31.95 | |
| Total (n) | 49028 | 1833 | 11223 | 435 | |
| % | 100 | 100 | 100 | 100 | |
| Evolution* | Cure | 96.34 | 88.36 | 91.67 | 76.74 |
| Death | 3.09 | 8.83 | 7.90 | 21.63 | |
| Death from other causes | 0.57 | 1.81 | 0.43 | 1.63 | |
| Total (n) | 51022 | 1823 | 11739 | 430 | |
| % | 100 | 100 | 100 | 100 | |
Source: Ministry of Health - SIVEP-Gripe data – June 14, 2021.
*Hospitalized patients only.
Final Considerations
This research aimed to collect and analyze data on COVID-19 and SARS cases in the Brazilian population of children and adolescents with disabilities throughout 2020. We considered 83.491 cases in children up to 19 years old. From this total, 2.730 (3.27%) were categorized with the disability proxy. The data have limitations regarding the possibility of generalization, since the registration in the Sivep-Gripe database, made available by the Ministry of Health and used in this research, is performed only for severe and confirmed cases.
Another limitation of the database that directly affects the debate about the population with disabilities is the lack of consideration of a variable that addresses the person with disabilities as advocated in the International Convention on the Rights of Persons with Disabilities, promulgated in Brazil by Decree No. 6949 (Brasil, 2009). Thus, although there is a variable in the database referring to trisomy XXI, the other disabilities were categorized on the basis of qualitative analysis of the terms entered by health teams in the descriptive morbidity field, which implies the consideration of only clinical terms. This restriction prevents us from generalizing the data and deepening the discussion on disability in a way that considers the necessary interactions between bodily impairments and the environment for its occurrence.
Despite these limitations, we sought, under the human development model of disability, to identify among the cases of SARS and COVID-19 the individual factors (age, sex, race); the types of disability (physical, hearing, visual, intellectual or psychosocial, and multiple); the required health resources (hospitalization, ICU admission, and use of ventilatory support); and the evolution of the case (cure, death, or death from other causes). The purpose of this research based on the human development model of disability is to enable the study and design of public policies that focus on improving the well-being of the population with disabilities, taking into account both the diversity of their bodies and the resources for access to health services, especially in the face of the epidemiological context, as well as environmental and structural factors relating to the communities and regions where they live.
When analyzing the cases, we observed that SARS concentrates 80% of the total cases, and most of them are children up to 9 years old. Regarding the age group of up to 4 years, there is considerable proportions between the cases of SARS - approximately 45%, - and COVID-19: at least 35% of the total, with the exception of children with hearing impairment. On the other hand, it is remarkable that a quarter of the COVID-19 cases occur among adolescents between 15 and 19 years old, especially those with physical disabilities. In this regard, we emphasize the need for preventive actions aimed at the particularities of the groups of children up to 4 years old and adolescents with physical disabilities.
Another factor that highlights the greater vulnerability of children with disabilities is the verification that all of them presented risk factors, with at least one morbidity (heart disease, chronic liver disease, asthma, diabetes, pneumopathy, obesity, and others), unlike those without disabilities, most of whom did not present any.
The progression of cases also points us to divergences among the groups: although in similar proportions of hospitalization in SARS cases, the proportion of children with disabilities infected by the coronavirus is higher, showing that 97% of them had to be hospitalized. And during these hospitalizations, the cases of children and adolescents with disabilities evolved significantly more to situations in which admission to Intensive Care Units and the use of ventilatory support were necessary, the latter reaching 67% of the cases. As for the final evolution of the hospitalized cases, we observed that more than 90% of the children without disabilities were cured of SARS and COVID-19. However, it is noteworthy that this percentage of cure decreases to 77% in the case of children and adolescents with COVID-19, who present the highest percentage of fatalities among the considered groups: 21% - more than the double of that found in relation to those without disabilities. In SARS cases, the proportion of children and adolescents with disabilities who die is three times that of those without disabilities: 9% and 3%, respectively.
In Brazil, the relationship between social inequality and the incidence of COVID-19 cases has been verified, and death from this disease became a considerable cause among fatalities of children and adolescents in poorer regions (Martins-Filho et al., 2021). On the other hand, the population of children and adolescents with disabilities are in a situation of social vulnerability, in households with lower income than other households, with less access to basic sanitation and education (Almeida, 2019). Accordingly, the data and analysis presented aim to contribute to the public policies necessary for the survival and well-being of children and adolescents in vulnerable situations, especially those with a disability, in the face of the epidemiological context of expansion of cases of COVID-19 and its new variants. Thus, we stress the importance of income-oriented public policies for the population, such as the Continuous Cash Benefit, and of planning other policies that include prioritizing not only persons with disabilities in the National Plan for the Operationalization of Vaccination against COVID-19 10, but also persons involved in their care networks - networks that are proving to be of great complexity and importance given the COVID-19 pandemic and all the recommended prevention measures.
Finally, we emphasize that the analyses show the differences between the cases and progressions among children and adolescents without disabilities and by types of disability, with the highest proportions of COVID-19 cases found among those with physical and intellectual or psychosocial disabilities. Considering age groups, we draw attention to the higher frequency of cases among children up to 4 years old, with intellectual or psychosocial disabilities between 5 and 9 years old, and those with physical disabilities between 14 and 19 years old. The progression of cases in children shows the relevance of considering their vulnerability and its effects on hospital facilities, since they are more likely to be hospitalized, to need Intensive Care Units and respiratory support. However, even with the use of these life-sustaining resources, the proportion of children with disabilities who die is twice as high (in cases of COVID-19) and three times as high (SARS) as those without disabilities. These findings ratify the need to consider disability as an important feature in discussions about social inequalities and public policies on access to health services, especially in the Brazilian context of pandemic expansion and the anomie of the federal entities responsible for its mitigation.
References
- Alam, J., & Bryant, W. (2016). Access to water and sanitation for people with paraplegia living in rural communities in Bangladesh. Physiology & Rehabilitation(3). https://doi.org/10.1080/2331205X.2016.1233686
- Alkire, S., & Foster, J. (2011a). Counting and multidimensional poverty measurement. Journal of Public Economics, 95(7), 476-487. https://doi.org/10.1016/j.jpubeco.2010.11.006
- Alkire, S., & Foster, J. (2011b). Understandings and misunderstandings of multidimensional poverty measurement. The Journal of Economic Inequality, 9(2), 289-314. https://doi.org/10.1007/s10888-011-9181-4
- Almeida, L. A. D. (2019). Deficiência e desigualdades no Brasil: pobreza, inserção no mercado de trabalho e renda. UFMG.
- Brasil. (1993). Lei nº 8.742, de 7 de dezembro de 1993. Dispõe sobre a organização da Assistência Social e dá outras providências. Retrieved from http://www.planalto.gov.br/ccivil_03/LEIS/L8742compilado.htm
- Brasil. (2004). Decreto nº 5.296 de 2 de dezembro de 2004. Regulamenta as Leis no 10.048, de 8 de novembro de 2000, que dá prioridade de atendimento às pessoas que especifica, e 10.098, de 19 de dezembro de 2000, que estabelece normas gerais e critérios básicos para a promoção da acessibilidade das pessoas portadoras de deficiência ou com mobilidade reduzida, e dá outras providências. Retrieved from http://www.planalto.gov.br/ccivil_03/_ato2004-2006/2004/decreto/d5296.htm
- Decreto nº 6.949 de 25 de agosto de 2009. Promulga a Convenção Internacional sobre os Direitos das Pessoas com Deficiência e seu Protocolo Facultativo, assinados em Nova York, em 30 de março de 2007., (2009). http://www.planalto.gov.br/ccivil_03/_ato2007-2010/2009/decreto/d6949.htm
- Lei nº 13.146, de 6 de julho de 2015. Institui a Lei Brasileira de Inclusão da Pessoa com Deficiência (Estatuto da Pessoa com Deficiência), (2015). http://www.planalto.gov.br/ccivil_03/_Ato2015-2018/2015/Lei/L13146.htm
- Diniz, D. (2017). Zica em Alagoas: a urgência dos direitos. LetrasLivres.
- Fietz, H., Mello, A. G. d., & Fonseca, C. (2020). Conexões íntimas e corporalidades singulares: deficiência em tempos de pandemia da Covid-19. Boletim Cientistas Sociais e coronavírus - ANPOCS, (61).
- Groce, N., Bailey, N., Lang, R., Trani, J. F., & Kett, M. (2011). Water and sanitation issues for persons with disabilities in low and middle-income countries: a literature review and discussion of implications for global health and international development. Journal of Water and Health, 09(4), 617-627. https://doi.org/10.2166/wh.2011.198
- Groce, N. E. (2009). Disability, poverty, human rights and the need for accurate data to promote action. Alter - European Journal of Disability research, Revue européen de recherche sur le handicap, 3(3), 185-187. https://doi.org/10.1016/j.alter.2009.05.002
- IBGE. (2018). Nota Técnica 01/2018: Releitura dos dados de pessoas com deficiência no Censo Demográfico 2010 à luz das recomendações do Grupo de Washington. Retrieved from ftp://ftp.ibge.gov.br/Censos/Censo_Demografico_2010/metodologia/notas_tecnicas/nota_tecnica_2018_01_censo2010.pdf
- Kittay, E. (1999). Love's Labor: essays on women, equality, and dependency. Routledge.
- Lodder, W., & Husman, A. M. d. R. (2020). SARS-CoV-2 in wastewater: potential health risk, but also data source. The Lancet Gastroenterology & Hepatology, 5(6), 533-534. https://doi.org/10.1016/S2468-1253(20)30087-X
- Martins-Filho, P. R., Quintans-Júnior, L. J., de Souza Araújo, A. A., Sposato, K. B., Souza Tavares, C. S., Gurgel, R. Q., Fontes Leite, D. C., de Paiva, S. M., Santos, H. P., & Jr, S., V. S. (2021). Socio-economic inequalities and COVID-19 incidence and mortality in Brazilian children: a nationwide register-based study. Public health, 190, 3. https://doi.org/10.1016/j.puhe.2020.11.005
- Mitra, S. (2006). The Capability Approach and Disability. Journal of Disability Policy Studies, 16(4), 236-247. https://doi.org/10.1177/10442073060160040501
- Mitra, S. (2017). Disability, Health and Human Development. Cham: Palgrave Macmillan. https://doi.org/10.2139/ssrn.3097355
- Mitra, S., Posarac, A., & Vick, B. (2013). Disability and Poverty in Developing Countries: A Multidimensional Study. World Development, 41(1), 1-18. https://doi.org/10.1016/j.worlddev.2012.05.024
- Mitra, S., & Sambamoorthi, U. (2008). Disability and the Rural Labor Market in India: Evidence for Males in Tamil Nadu. World Development, 36(5), 934-952. https://doi.org/10.1016/j.worlddev.2007.04.022
- Mizunoya, S., & Mitra, S. (2013). Is There a Disability Gap in Employment Rates in Developing Countries? World Development, 42(1), 28-43. https://doi.org/10.1016/j.worlddev.2012.05.037
- Mizunoya, S., Mitra, S., & Yamasaki, I. (2018). Disability and school attendance in 15 low- and middle-income countries. World Development, 104, 388-403. https://doi.org/10.1016/j.worlddev.2017.12.001
- Nussbaum, M. C. (2013). Fronteiras da justiça: deficiência, nacionalidade, pertencimento à espécie (S. d. Castro, Trans.; E. W. M. Fontes, Ed.). (Frontiers of Justice)
- Ranzani, O. T., Bastos, L. S. L., Geli, J. G. M., Marchesi, J. F., Baião, F., Hamacher, S., & Bozza, F. A. (2021). Characterisation of the first 250 000 hospital admissions for COVID-19 in Brazil: a retrospective analysis of nationwide data - The Lancet Respiratory Medicine. The Lancet. Respiratory medicine, 9(4), 12. https://doi.org/10.1016/S2213-2600(20)30560-9
- Schuch, P., & Sarreta, M. (2020). Deficiência, Coronavírus e Políticas de Vida e Morte. Boletim Cientistas Sociais e coronavírus - ANPOCS, (35).
- Sen, A. (2009). The Idea of Justice. The Belknap Press of Harvard University Press. https://doi.org/10.2307/j.ctvjnrv7n
- Trani, J.-F., Bakhshi, P., Brown, D., Lopez, D., & Gall, F. (2018). Disability as deprivation of capabilities: Estimation using a large-scale survey in Morocco and Tunisia and an instrumental variable approach. Social Science & Medicine, 211, 48-60. https://doi.org/10.1016/j.socscimed.2018.05.033
- Trani, J. F., & Loeb, M. (2012). Poverty and disability: A vicious circle? Evidence from Afghanistan and Zambia. Journal of International Development, 24(supplement S1), S19-S52. https://doi.org/10.1002/jid.1709
Endnotes
-
For more information: https://censo2010.ibge.gov.br/ and https://ftp.ibge.gov.br/Censos/Censo_Demografico_2010/metodologia/notas_tecnicas/nota_tecnica_2018_01_censo2010.pdf.
Return to Text -
The 2010 census identifies as people with disabilities those who had at least one affirmative response to the question about having great difficulty hearing/seeing/walking or climbing steps. This parameter does not apply to the question regarding mental/intellectual disability because the response categories are "yes" or "no" (IBGE, 2018).
Return to Text -
The Continuous Cash Benefit (BPC), provided for in the Organic Law of Social Assistance - LOAS, is the guarantee of one minimum wage per month to the elderly aged 65 or over or to persons with disabilities of any age (Brazil, 1993). In the case of the person with disability, his/her condition, according to the Ministry of Citizenship, must cause long-term physical, mental, intellectual or sensory impairments (with effects for at least two years), which prevent him/her from participating fully and effectively in society on an equal basis with others. To be entitled to BPC it is mandatory that the income per person in the family group be less (or less) than a quarter of the minimum wage. More information at: https://www.gov.br/cidadania/pt-br/acoes-e-programas/assistencia-social/beneficios-assistenciais-1/beneficio-assistencial-ao-idoso-e-a-pessoa-com-deficiencia-bpc.
Return to Text -
More information at: https://www.ibge.gov.br/estatisticas/sociais/saude/9160-pesquisa-nacional-de-saude.html?=&t=o-que-e .
Return to Text -
Anis is a non-profit, non-governmental organization focused on research, advisory and training in bioethics in Latin America. Based in Brasilia, it develops its activities with a multidisciplinary team of professionals with extensive experience in social research, political advocacy, strategic litigation, and communication projects on violations and defense of rights in fields such as sexual rights, reproductive rights, disability, mental health, violence, and criminal and socio-educational systems. More information at https://anis.org.br/.
Return to Text -
The databases are available at: https://opendatasus.saude.gov.br/dataset/bd-srag-2020, Accessed in June, 2021.
Return to Text -
The data dictionary of the Sivep-Gripe database is also available on the Ministry of Health's website: https://opendatasus.saude.gov.br/dataset/9f76e80f-a2f1-4662-9e37-71084eae23e3/resource/b3321e55-24e9-49ab-8651-29cf5c8f3179/download/dicionario-de-dados-srag-hospitalizado-27.07.2020-final.pdf
Return to Text -
On September 4, 2020, bill 2179/2020 was presented to the House of Representatives, amending Law no. 13. 979, of 02/02/2020, which "provides on the measures for facing the public health emergency of international importance due to the coronavirus responsible for the outbreak of 2019", to dispose on the registration and availability of information of epidemiological interest regarding patients with suspected or confirmed coronavirus infection seen in public and private health services, including data related to ethno-racial markers, age, sex, and disability status. More information on this subject can be found at: <https://www.camara.leg.br/proposicoesWeb/fichadetramitacao?idProposicao=2262096> .
Return to Text -
We emphasize that due to the small number of cases considered as a proxy for disability among children and adolescents with disabilities it was not possible to perform the analyses regarding the population rates of infection and mortality.
Return to Text -
Available in: https://www.gov.br/saude/pt-br/media/pdf/2021/janeiro/29/PlanoVacinaoCovid_ed4_15fev21_cgpni_18h05.pdf
Return to Text
