
Research on geographic mobility in the US has neglected disabled people, missing their experiences of abridged citizenship as their desires to move across states are frustrated by social policy barriers. To illustrate how meso- and macro-level factors impact individual lives, I review three publicly-reported stories of Medicaid home and community-based services (HCBS) users. To advance research in this area, I analyzed these three stories and developed an original conceptual model, Moves in Context. The model attends to the individual cross-state move trajectories of disabled people, and HCBS users, in particular. Moves in Context focuses on the individual journey (i.e., impetus, ability, and success of move; and the influence of the move story) in relation to both social position/personal resources and social structure/ideology. Through the model, I introduce and explain intrastate confinement, a term to describe the geographic immobility resulting from policy variations across states. I conclude with a discussion of the broader implications of both the Moves in Context model and intrastate confinement for further research on disabled people and interrogating other social problems.
"No social study that does not come back to the problem of biography, of history and of the intersections within a society has completed its intellectual journey."
"If disability is conceptualized as a terrible unending tragedy, then any future that includes disability can only be a future to avoid. A better future, in other words, is one that excludes disability and disabled bodies; indeed, it is the very absence of disability that signals the better future. The presence of disability, then, signals something else: a future that bears too many traces of the ills of the present to be desirable."
In this paper, I propose a conceptual model through which to research the cross-state migration pursuits of disabled people, and specifically the structurally (re)produced barriers to these moves for those who use Medicaid home and community-based services (HCBS). Bridging sociological theory as argued by Mills (1959) and current thinking in disability studies vis a vis (Kafer 2013), I argue that these moves are more than the mundane biographical events and require examination within the context of social structures at the meso- (state policy and politics) and macro- (institutionalized, State-supported ableism) levels. Given the general lack of available data and research in this area, I engage three publicly available media accounts of frustrated cross-state move attempts of disabled Medicaid HCBS users to identify elements for generating social problems theory. Informed by these stories, I generated an "ideal type" conceptual model, Moves in Context, which has both the flexibility to describe many specific, situated experiences of cross-state moves and the analytic heft to examine the patterning of these experiences as (re)produced through social, political, cultural, and economic structures. I describe this model and a new concept that emerges through it, intrastate confinement, the social phenomenon of immobility experienced by disabled people (and others) and accompanying risk for differential citizenship when pursuing cross-state moves that arises from interstate variation in social policy. I conclude by addressing the utility of Moves in Context and intrastate confinement for future theoretical inquiry, empirical research, and social change.
Cross-State Mobility for Disabled People: A Social Problem
In the US, barriers to cross-state mobility for disabled people are a social problem. Indeed, I argue this problem is socially produced, constructed, maintained, and experienced. This is especially true for those who qualify for and use Medicaid home and community-based services (HCBS) for assistance leading meaningful lives in the community pursuing their self-determined educational, employment, and social goals.
Barriers to cross-state mobility for disabled people arise not from divine law nor biological phenomenon, but rather result from the socially produced rules that people (i.e. policymakers) have developed to distribute resources (Albrecht 1992; Stone 1984). As products of a bureaucratic system, these barriers have emerged from the workaday functioning of society. In conflict with an obligation to increase disabled people's opportunities for community living and meaningful social participation, Medicaid's structure as a fiscal partnership between states and the Federal government produces barriers to cross-state movement due to the resulting variation in program administration and offerings by state, known as interstate variation (Olmstead v. L.C. 1999; Office of the Secretary 2015).
These barriers are socially constructed as non-problematic or the "way things are" based on a series of related constructions of disabled people, the State, and corporeality (Albrecht 1992; Kafer 2013; Stone 1984). Based on the ways that policies are written and carried out, disabled people are socially constructed as program users, presumed to be and (re)presented as immobile, as rooted in one state and, consequently, eligible only for programmatic support from that state (Murinko 2014; Ruiz 2013; Scott 1981). The unintended consequence, then, is that disabled people are cast as undesiring and undeserving of cross-state mobility, and ungrateful or unruly if expressing frustration at barriers to mobility.
These barriers (and related constructions) are socially maintained via the actions of people with power to respond to evaluative or redistributive rules (Lipsky 1983; Stone 1984). Disabled people who wish to cross states are confronted with an obdurate reality of how these social programs work and how users of these programs are expected to behave (Murinko 2014; Ruiz 2013; Schwalbe 2007). At the very least, the social maintenance of these barriers to cross-state movement is merely the continuation of the status quo. Even if disabled people were presumed to be immobile when Medicaid first began to offer HCBS in 1981, more than three decades of societal and policy shifts should have signaled an interest in change (e.g., Olmstead v. L.C. 1999; Burwell 2015) affirming the rights of disabled people to pursue social, educational, and economic participation. Despite nearly two decades of bills introduced to change the structure of Medicaid to create a shared "policy floor" across all states which would indirectly address these issues of geographic mobility, both the presumed immobility of disabled people and the self-evident inappropriateness of state programs following "bodies" and crossing state lines remain entrenched (Grossman 2011). And in fact, there seems to be more support than ever for state control of Medicaid (i.e., block grants; H.R. 1628 115th Congress 2017; Ryan 2016), a plan that would not only maintain but enhance these barriers to cross-state movement, by increasing the disparities in services available across states and reducing allocations over time (Congressional Budget Office 2017; Shapiro et al. 2016; Solomon 2017) .
These processes combine to structure the social experiences of limited cross-state mobility: at the collective level, as a form of targeted discrimination and as an impingement on full and equal social participation that, later in this paper, will be described as intrastate confinement. Paying attention to these social experiences involves disentangling the "imagined futures" presumed for disabled people by those who design and implement these policies (i.e., potential life paths as predicted or envisioned by others) from those futures that disabled people imagine and determine for themselves (Kafer 2013). Additionally, it requires understanding that these futures, as planned and enacted by disabled people, are more than merely biography but also distinct products of history; not just personal troubles but indeed a significant public issue (Mills 1959).
Medicaid Home and Community-Based Services (HCBS)
Medicaid is the primary payer for home and community-based services (HCBS) in the United States (Ng et al. 2016). After being deemed eligible, disabled individuals gain access to public funds that pay for technology, services, and care workers to facilitate community living, including assistance with activities of daily living (e.g., eating, bathing, toileting, grooming, dressing, and transferring in/out of beds and wheelchairs, Katz et al. 1970); and instrumental activities of daily living (e.g., financial management, light and heavy housework, using the telephone, traveling to and from work/other appointments, food shopping and meal preparation, and medication management, Lawton and Brody 1969). In 2013, HCBS accounted for $75 billion, or nearly 1 in 6, of all Medicaid dollars spent that year (Eiken et al. 2015). These services help approximately 3 million people avoid unnecessary and undesired institutionalization (Ng et al. 2016).
In the absence of HCBS, program users would not be able to continue their lives in the community, losing access to educational, employment, and social opportunities. Disabled people consistently communicate their desires to live in the community rather than nursing homes, as evident in research and political organizing (ADAPT 2018; Caldwell 2007; Caldwell and Heller 2007; Grossman et al. 2007; San Antonio et al. 2009; Simon-Rusinowitz et al. 2001). Since 1997, there has been consistent political pressure from disability rights social movement organizations to standardize and increase access to Medicaid HCBS as evidenced by the repeated introduction of bills to this effect, including the Medicaid Community-based Attendant Services Act of 1997 (H.R. 2020 105th Congress [1997]) and most recently the Disability Integration Act of 2017 (ADAPT 2018; Grossman 2011; Schumer 2017).
Interstate Variation in Medicaid HCBS
Although the number of Medicaid HCBS users has increased over the last decade (from 2.1 to 3 million) program users continuously report unmet needs in access to and adequacy of Medicaid coverage for these services (Kaye, Harrington, and LaPlante 2010; LaPlante et al. 2004). Access to HCBS is not evenly distributed across states due to the state-federal matching structure of Medicaid funding and weak federal regulations. The HCBS programs used by the greatest number of users are considered optional for states and are not equivalent across states — only 32 states offer optional benefits in their Medicaid state plans and the over 289 HCBS waivers are unevenly spread across 47 states (Ng et al. 2016). While the majority of HCBS are merely optional under Medicaid, states are under some pressure to increase the availability of these options as a result of (Olmstead v. L.C. 1999). This Supreme Court ruling found that states have a legal obligation, under Title II of the Americans with Disabilities Act, to use Medicaid dollars to fund HCBS so that disabled people have the opportunity to live in the "most integrated setting appropriate to the needs of qualified individuals with disabilities" (28 CFR § 35.130(d), 1998; Olmstead v. L.C. 1999).
Despite this judicial ruling, researchers have consistently documented interstate variation, the uneven and disparate distribution of these services across states. Interstate variation in Medicaid HCBS has been reported for: services and technology covered, across all beneficiaries and by disability type; expenditures, overall and per capita; the criteria for, and processes of, evaluating eligibility; and the strategies for restricting access, including waiting lists and restrictive financial eligibility criteria (Kassner et al. 2008; Kassner and Shirey 2000; Kitchener, Ng, and Harrington 2007; LeBlanc, Tonner, and Harrington 2000; Reinhard et al. 2014, 2011; Summer and Ihara 2005; Wenzlow et al. 2013). However, research has not contended with the effect of interstate variation in Medicaid HCBS on the cross-state mobility patterns of program users, or disabled people and their families, more broadly.
Geographic Mobility in the US
In 2015, nearly 7.5 million people, about 2.4% of the population of the US, had engaged in a cross-state move in the previous year (United States Census Bureau 2015). To illustrate the macro-level implications of these moves, data has been visually depicted in terms of net population gains or losses within states, as well as the traffic between any two particular states (Aisch, Gebeloff, and Quealy 2014; Ingraham 2015; Mason 2013). Other research has highlighted gender differences and racial disparities in cross-state moves (Ihrke 2014; Ihrke and Faber 2012). However, limited research has examined cross-state movement in terms of disability, and many do not focus on adults with disabilities in the working years (Conway and Rork 2011; Graefe, De Jong, and May 2006; Mateyka 2015; Sharma 2011, 2013).
Geographic Mobility for Disabled People in the US
Despite this limited body of research, there is initial evidence that disabled people and their families are likely to experience disparities in access to cross-state moves and confront structural barriers to accessing community living within the policy systems and programs of which they are a part. One study focused on relocation found that a greater percentage of disabled people reported a desire to move, both within and across states, because of residential dissatisfaction than their nondisabled counterparts (12.5% v 8.2%). However, disabled people who desired moves were less likely (17.3%) to move than nondisabled people with similar desires (19.0%), and people with physical and communicative disabilities were even less likely to do so (16.4% and 15.8%, respectively; Mateyka 2015).
In another study, families that included a person with a disability were found to be significantly less likely to move out of state than families without a disabled member, except in states where Temporary Aid for Needy Families (TANF) policies were so restrictive that they acted to "push" families with disabilities to migrate to other states (Graefe et al. 2006). By contrast, Conway and Rork (2011) found that among older adults, those who migrated across state lines reported higher rates of disability than those who did not. This type of move, described as "assistance migration," allows older adults to move closer to family for support. This is consistent with research that found that as health problems increase for older adults, so does the likelihood that they will move to be closer to family (Litwak and Longino 1987).
Sharma (2011) found further evidence for (Litwak and Longino 1987) "second-move" hypothesis (i.e., that older adults with functional limitations or health issues are likely to move again, to locate nearer to social support) by examining older adults from Florida by disability status. They found that both those with mobility limitations (e.g., difficulty getting out of the house) and those with personal care limitations (e.g., difficulty getting around inside the home or with dressing or bathing) were more likely to move than those without either limitation. Older adults with mobility limitations, however, were more likely to move out of state, while those with personal care limitations were more likely to move within the state of Florida. Other research by Sharma (2013) illustrated that, contrary to expectation, older adults with disabilities also engage in "amenity moves" when residing in states that are part of a "chain migration" pathway: a pattern of migration that links two states such that outmigration from one leads to high levels of inmigration to another that is a desirable retirement destination (e.g., nice weather, social opportunities). Both older adults with physical disabilities and those with cognitive disabilities living in chain migration states were more likely to engage in cross-state moves to either Florida or Arizona than nondisabled adults from other states, and at rates nearly similar to their nondisabled counterparts in their states of origin.
Geographic Mobility, Disability, and Citizenship
Examining geographic mobility from a disability rights perspective supports an investigation into how barriers to cross-state mobility may be an infringement upon full citizenship for disabled people. This approach begins to place disability within embodied experience, recognizing bodies as mobile across geography (Hughes and Paterson 1997; Sherry 2016). It also attends to the social conditions that (re)produce and (re)act toward bodily and behavioral difference (Oliver 1983; Oliver and Barnes 2012; Thomas 2004). Such an analysis addresses corporeal, or bodily, mobility – the literal ability for people to physically move between and across locations (Urry 2000a). Given that many forms of social participation in modern societies require bodily presence, it is necessary to interrogate the structures that act as barriers to this form of mobility, unevenly producing and patterning immobility for certain citizens (Cass, Shove, and Urry 2005; Urry 2002, 2000b).
Throughout US history, disabled people have had their social, civil, or political rights as citizens systematically denied (Baynton 2001; Marshall 1950; Nielsen 2012). Disabled people have struggled to claim these rights, (re)negotiating with local, state, and federal levels of government (i.e., the State as an apparatus) and (re)constructing their position as agentive citizens and building effective coalitions (Barnartt and Scotch 2001; Carey 2009; Christiansen and Barnartt 2003; Fleischer and Zames 2011; Pelka 2012; Scotch 2009). Religious, medical, and legal discourses each contribute to the degradation and delegitimization of disabled people's experience of citizenship, resulting in a second-class citizen status enshrined by the State through law and practice (Carey 2009; Liachowitz 1988; Schweik 2010; Stone 1984). For many disabled people in the US, the State's presence in their daily lives is most acutely felt through Medicaid, a social program focused on the interface of health and poverty.
Cross-State Moves by Medicaid HCBS Users: Three Accounts
Theorizing cross-state mobility for disabled people is challenged by a combination of poor data collection systems and a limited body of research (summarized above). I located three publicly-reported media accounts of Medicaid HCBS users who experienced failed cross-state move attempts. In each of these cases, I found that the state-by-state patchwork of Medicaid HCBS programs that results from interstate variation creates a structural barrier to cross-state movement uniquely borne by program users. In this section, I summarize these three stories to illustrate how interstate variation has material and social consequences for program users desiring, planning, and pursuing cross-state moves.
The first story recounts the experiences of Zach Sayne who lived in Georgia as a young boy with cerebral palsy and seizures who was nonverbal and partially blind. At age ten, after Zach began using a feeding tube, his mother sought help supporting him after school while she was at work. He was denied access to local afterschool programs. Furthermore, the state's Medicaid program was unwilling to fund an assistant to help him remain at home, the form of caregiving support that would have facilitated his mother's ability to continue to work. The state did, however, offer to pay the full cost of Zach's care in a nursing home. And yet, the only nursing home willing to provide Zach with care was in Alabama, where he eventually moved, far from his home and family. Years later, when his mother, Nola, tried to move him back to Georgia, he was denied access to the state's Medicaid program because now as an adult, he was no longer a resident and therefore not eligible. She was given the opportunity to become his legal guardian and to reapply for services in Georgia, but there were two problems: 1) there was a waiting list for these services and 2) while on the waiting list, Zach would need to be housed in a Georgia nursing home, none of whom were willing to accept a young man. Unfortunately, he died at the age of 25, in a nursing home in Alabama, 200 miles away from his mother (Shapiro 2013).
The second story involves Ashley Volion, a Medicaid HCBS user who uses personal care attendant (PCA) services provided through a waiver program in Louisiana. She applied for and was admitted to a doctoral program in Disability Studies at a public university in Illinois. She intended to move to Illinois for her degree and return to Louisiana after completing her studies. Ashley received dispensation to have her care workers come with her to Illinois for 30 days to help her with the cross-state move transition. However, she became caught between the two states: Louisiana refused to pay for services during her studies while Illinois would only allow her access to PCA services after she had been living in the state for one year. Because there was a waiting list for them, there was no guarantee these services would be available. She eventually decided the educational and social benefits of a cross-state move did not outweigh stable and sustainable access to PCA and is pursuing her degree through a modified distance program (Ruiz, 2013; A. Volion, personal communication, February 9, 2017).
The final story belongs to Shawn Murinko, a lawyer from Washington state who applied for and was offered a job in the U.S. Department of Justice, an opportunity he described as his idea of the "perfect job". The job required a move to the state of Maryland, which has different Medicaid programs and policies than his home state. In Washington, he had access to PCA to assist with activities of daily living through Medicaid. However, the new job would provide earnings above the income cap for Maryland's Medicaid program and the state would expect him to devote over $100,000 to pay for the same services that had been funded by Washington state. This would effectively leave less than 10% of his salary for other expenses, limiting his ability to contribute financially to his household, which included a wife and two children. Despite working with his U.S. Senator, no solutions were found. Consequently, he remained in Washington with his family, frustrated by his inability to move and painfully aware that the inequity that he experienced is a byproduct of interstate variation in Medicaid HCBS (Murinko 2014).
State variation in Medicaid HCBS programs and lack of portability of these services across state lines negatively impacted the educational, economic, and social opportunities for each of these program users. Table 1 provides a summary of these cross-state move stories, detailing the states involved, the impetus for the move, and the outcome/impact on the lives of the individuals Medicaid HCBS users attempting to move. For Zach Sayne, his body could place certain demands upon the State in Alabama that it could not in Georgia – or rather these demands were met with variable responses, directly impacting his ability to participate in family life as a child, an adolescent, and a young man. The programs that impacted Zach's life had not imagined for him a future that included living in the community (necessitating the first move) nor one that involved a cross-state move for family reunification (resulting in his continued geographic displacement from his family). For both Ashley Volion and Shawn Murinko, interstate variation in Medicaid HCBS presented barriers to cross-state movement that led them to feel "stuck" in their current state of residence, a phenomenon that I have labeled intrastate confinement (more below). The irony is that these experiences are embedded within and emerge indirectly from Medicaid HCBS, the very programs created to support community living.
| Program User Name (States involved) | Impetus for moving | Outcome |
|---|---|---|
| Zach Sayne (GA, AL) | Move closer to family | Unable to move to destination state, died in other state hundreds of miles from family |
| Ashley Volion (LA, IL) | Attend graduate school | Unable to attend doctoral program in-state; Accommodated with distance program, remains in initial state |
| Shawn Murinko (WA, MD) | Advance career | Unable to accept higher-paying job, remains in initial state |
A Conceptual Model of Cross-State Movement for Medicaid HCBS Users
Despite the three publicly available and emotionally evocative accounts of barriers to cross-state moves for disabled Medicaid HCBS users, scant attention has been paid to this issue in the disability policy or demography literature. In this section, I use the three vignettes above as the basis for an active theorizing of cross-state movement (and barriers thereof) as a social problem, outlining the elements of individual's move trajectories and how both social position and social structure influence these trajectories.
As part of the theorizing process, I committed to ensuring the Medicaid HCBS user remained the focal point of the analysis. Table 2 illustrates the autonomy of the program users varies across twelve general reasons for cross-state moves by addressing three questions for each: 1) was the move driven by their pursuit of opportunity or necessity? 2) was the move self-determined, determined by the actions of another, or a change in circumstance? and 3) what level of control does the user have over the moving process? These reasons for moving reflect the three stories above, the experiences of disabled people in the wake of Hurricane Katrina and other natural disasters resulting in displacement, the gerontology literature, the research on familial transition in caregiving roles for adults with intellectual disabilities, and informal conversations I had with disabled people and their family members. The list is intended to be illustrative rather than exhaustive. Each reason for moving represents one potential starting point in the conceptual model I developed. Figure 1 presents the complete model, entitled Moves in Context, a tool for charting individual move trajectories and identifying patterns across groups of stories, attentive to the influences of both social structure and personal resources on the (potential) moves of disabled people.
| Impetus for move | Program user's move is driven by… | Program user's move is determined by… | Program user's perceived level of control |
|---|---|---|---|
| Desire for social outlets (including dating) | Opportunity | Self | High |
| Desire for disability culture/community | Opportunity | Self | High |
| Desire for college degree (or beyond) | Opportunity | Self | High |
| Desire for internship, job, increased wages | Opportunity | Self | High |
| Deinstitutionalization | Opportunity | Self | High |
| Change in health status | Necessity | Self | Limited |
| Increased access to direct care workforce | Necessity | Self | High |
| Residential displacement (includes natural disasters) | Necessity | Situation | Limited |
| Military transfer | Necessity | Family member | Limited |
| Co-residing family member retirement/death | Necessity | Family member | Limited |
| Co-residing family member pursuit of economic opportunity | Necessity | Family member | Limited |
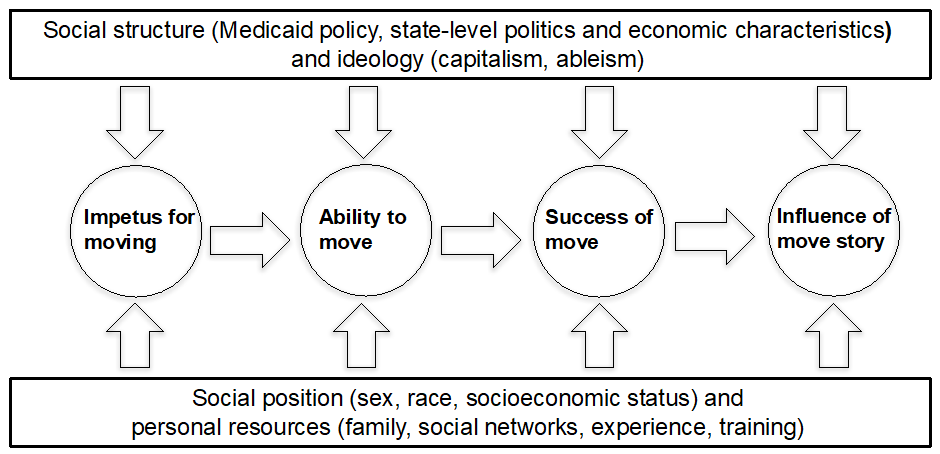
Figure 1. Moves in context: A model of cross-state movement dynamics for Medicaid home and community-based services (HCBS) users. The model illustrates how social structure/ideology and social position/personal resources influence individual trajectories of Medicaid HCBS users pursuing cross-state moves. In the center of the model are four circles connected by right-facing arrows that represent an individual cross-state move trajectory: 1) impetus for moving; 2) ability to move; 3) success of move; and 4) influence of move story. Arrows point at each of these four circles from both below and above to indicate how individual trajectories are influenced from both sets of factors. The arrows from below emanate from a box representing social position/personal resources while the arrows from above point downward from a box representing social structure/ideology.
Moves in Context: A Conceptual Model
Both social position/personal resources (the bottom box) and social structure/ideology (the top box) are depicted in the Moves in Context model as influences on the cross-state move behavior and experiences of disabled people. Social position includes demographics, identity, and other forms of social positionality (e.g., class, sexuality, disability) whereas personal resources refer to the benefits of social experience and access to social networks, including families, community organizations, and online groups. Both social position and personal resources are evaluated at one moment in time (i.e., a snapshot) but reflect an accumulated lifetime of experience and might change, expand, or shrink during the time period when one is considering a move (O'Rand 1996). Personal resources are not evenly distributed across populations and social position shapes their availability and the avenues to access them.
Personal resources are relevant to, accessed as part of, and consequently exert influence over, each of the steps along an individual's movement trajectory. For example, social positions and personal resources shape how, why, and when one: learns about opportunities that include cross-state moves; is encouraged to, or seeks support for, a future that involves a cross-state move, determines the pros and cons of opportunities that require a cross-state move, evaluates the likelihood that cross-state moves will be successful or sustainable, procures temporary housing as one plans the move, requests help with physical labor or travel from friends or family, relies on friends and family to address service gaps as one navigates the switch across state HCBS systems, strategizes how to sustain the move while experiencing significant obstacles in the new state, and disseminates their tale as either one that is cautionary or encouraging.
Whereas social position and personal resources are things that individuals draw from, social structure refers to the milieu in which individuals are embedded, shaping and constraining action, and its influence becomes present through both ideology (e.g., capitalism and institutionalized ableism, sexism, and racism), and the consequent distribution of resources via the State through federal, state, and local law, politics, policy, and practice. Acknowledging the significance of the organization of society via capitalism attends to both the social production and social construction of disability (Albrecht 1992; Russell 1998). Additionally, identifying the role of institutionalized ableism as it influences macro-level structure provides an opportunity to look at how this ideology affects both individuals and the social situations in which they are embedded. As with social position and personal resources, social structure and ideology influence each of the four steps along an individual's path to move across states. For example, social structure and ideology impact how, when and why potential or pursued cross-state moves for disabled people are possible. These factors influence: the social, political, and economic distribution of opportunity versus necessity, the possibility of cross-state moves for those who experience residential dislocation due to personal tragedy or natural disaster, the self-assessment of whether or not one is able to move, the pursuit of a cross-state move as imagined or intended, the evaluation of success by both the individual and the systems/programs which they are a part, and the description of the move story to other program users through formal or informal channels.
Attention to social structure allows for an interrogation of the fiscal crises of the State and the welfare state (O'Connor 1973; Offe 1984) and the political reframing of austerity in social spending as both rational and even "compassionate" despite the human cost to disabled people and their families. By reducing conversations about civil rights to discussions of economics, this austerity frame supports both the enduring institutional bias in Medicaid funding 1 and the inherent necessity of interstate variation in service access and type as a result of scarcity. Consequently, an individual who wishes to move across states (e.g. to pursue an educational or employment opportunity) is confronted with both explicit attitudinal barriers and implicit ones embedded in the very policies that offer the possibility of movement in the first place (Hahn 1988; Kafer 2013).
For adults with disabilities who use Medicaid HCBS, and by extension, the family members who provide supports and services and/or with whom they reside, interstate variation is one manifestation of social structure that exerts strong influence over potential move trajectories. Operating at the meso-level, interstate variation results from the federal/state matching structure of Medicaid funding. However, it is further nurtured as a social force impacting the lives of HCBS users by macro-level ideologies that pit states against the federal government in support of ideas like local control of schools in conflict with federal legislation (i.e. the Individuals with Disabilities Education Act), and block grants for social services (such as those proposed for Medicaid). Another outcome of this ideology is the positioning of the federal government as a distributor of incentives to encourage reticent states to take advantage of programs that would expand access to a larger number of qualifying citizens with disabilities (e.g., Medicaid expansion, the Community First Choice Option).
Charting the Move
The pathway describing the potential, "ideal type" journey for cross-state moves has four parts: 1) impetus for moving, 2) ability to move, 3) success of the move, and 4) influence of the move story. For visual ease, it is depicted as a continuous, linear trajectory. Representing the model this way also offers analytic clarity when looking at cross-state move pursuits as discrete journeys, refocusing on actions taken by disabled Medicaid HCBS users. However, when charting particular experiences, the pathway may include false starts and multiple assessments of resources or ability before a move occurs, leading to offshoots and branches from the main artery.
Impetus for moving
Understanding the impetus for moving recognizes the larger social situation in which the individual is embedded and how that situation affects their framing of a potential move. The variety of reasons why a Medicaid HCBS user might plan or pursue a cross-state move can be collapsed into two general categories: moves may occur in response to opportunity or necessity. In either case, another person's move story may have influenced the move – something that is not easily captured in the linearity of the model.
Moving to pursue opportunity. In this model, opportunity, as distinguished from necessity, is a motivating factor for a cross-state move that has the expected result of adding value (educational, economic, social) to the HCBS user's life experience. Cross-state moves pursued as responses to opportunity are concordant with the concept of self-determination, pointing to the agency of disabled individuals as they seek and follow desired opportunities for educational, economic, and social benefits (Murinko 2014; Ruiz 2013). Given the changing legal and programmatic landscape to enhance educational and employment outcomes for disabled people in the US, one would anticipate that there would be increased opportunities worthy of pursuing and that, especially for young disabled people growing up in the post-ADA world, these would be part of the futures they imagine for their adult lives (Leiter 2012). Social benefits include moving to a new area to be closer to family, friends, or potential or current dating partners. Other benefits might include access to infrastructure that supports accessing these new social opportunities: public transit, accessible public spaces, and housing options that meet visitability standards (NCIL 2018). They might also involve access to disability culture and community, rich sources of informational, instrumental, and social support, in areas of the country that played significant roles in the Disability Rights Movement (e.g., Berkeley/San Francisco, Chicago, etc.).
Moving out of necessity. Cross-state moves driven by necessity can be broken down into three subcategories: 1) those that are self-determined; 2) those determined for an HCBS user by a family member; and 3) those that are determined by an external situation. Moves that are self-determined include when someone moves closer to family/friends on whom they might call for extra paid or unpaid support. These moves involve self-assessment by HCBS users and the realization that either they have greater assistance needs than are currently being met or that they cannot access the appropriate level of support via the direct care workforce available in their state. The former is similar to "assistance moves" described in the gerontological literature (Litwak and Longino 1987), while the latter is an example of a geographically-bound social environment disabling an individual as in the "social model" of disability (Oliver 1983; Oliver and Barnes 2012). In both cases, the macro-structure precipitates the move but the decision is directed/determined by the individual – they retain agency while responding to challenges arising from social structure.
By contrast, moves determined for HCBS users by family members highlight the nested context of the lives of many Medicaid HCBS users and other disabled people who either co-reside or live near family members who provide services and supports, paid and/or unpaid. These cross-state moves are initiated in response to changing circumstances for the family members, who may be pursuing educational, economic, and social advancement, or planning for or responding to a significant shift in the current family caregiving dynamic (e.g., co-resident parent no longer able to provide services and supports; selling of family home after co-resident parent dies). In these cases, Medicaid HCBS users have limited control over the move and may have preferences that are either unexpressed or unable to be accommodated due to family finances or established social roots elsewhere.
Lastly, moves determined by an external situation (i.e., an emergency) reflect the specific interactions between personal resources and social structure for that individual. Throughout the experience of residential dislocation the HCBS user's level of control is limited even if they are moving on their own (rather than a family member's insistence). When the emergency circumstances are more contained (as in the case of a house fire), individuals pursuing cross-state moves may rely more heavily on personal resources and feel resistance from social structures (including interstate variation). In other circumstances where the emergency is more widespread, as in a natural disaster, it is possible that there will a stronger structural response that may ease the reliance on personal resources and networks.
For Zach Sayne, the initial move happened not out of desire (his or his mother's) but rather out of necessity and constraint. That is, her economic need to work and his need for safe after school care necessitated access to HCBS, which he was denied. The only remaining alternative, though undesirable, required geographic dislocation from family and community. By contrast, the request for the second move (returning to Georgia) was driven by desire for family reunification, even though it was not achieved. For Ashley Volion and Shawn Murinko, the reasons for the move were directly related to the desire to pursue opportunities: education in the former case and economic/occupational advancement in the latter. Both of these examples highlight the disconnect between Medicaid HCBS policies that prevent cross-state moves and the stated goals of other disability policies to increased educational access and employment outcomes.
Ability to move
In this model, the ability to move is self-assessed as Medicaid HCBS users evaluate the feasibility of a cross-state move. There is a reciprocal consideration of the impetus to move in relation to the ability or capacity to move. Arriving at the decision (not) to move involves an assessment of both social structure and personal resources to see if a successful cross-state move could be imagined before it is undertaken. Assessments of capacity include both an audit of personal resources that offer support for planning and implementing the move and research on the structural elements that might impact the move to identify potential barriers and solutions, as well as to identify new avenues for information or assistance.
For Zach Sayne, the ability to return to Georgia from Alabama was measured against structural constraints which proved to be too great to overcome; thus, the move did not occur. The combination of waiting lists and the lack of temporary residential placement for a man of his age resulted in the symbolic walls between the two states materializing as physical barriers to cross state movement. For Ashley Volion, the ability to move from Louisiana to Illinois was evaluated in terms of access to personal care attendants – either to pay for her attendants from Louisiana in Illinois or to qualify in Illinois to access attendants in that state. Despite petitioning an administrative law judge in her home state and exploring options to move on to the personal care attendant program in the new state, she was not able to overcome the structural obstacles presented by interstate variation and consequently, she remained in Louisiana. Similarly, Shawn Murinko evaluated his access to personal care attendants – in terms of how the cost of these services would be distributed. If he were to move to Maryland for this ideal job, the accompanying pay raise would be eaten up by out-of-pocket costs for services since his income would disqualify him from Medicaid HCBS eligibility in that state. In fact, the responsibility for these services would fall so directly on his shoulders that his family income would be negatively impacted by the move and new job. For him, the decision to move was thwarted not only the lack of portability of these services across state lines but also by anticipated economic penalty.
Success of move
The success of the move operates at two levels. First, Medicaid HCBS users will evaluate their own cross-state move experience to determine if they met their intended goal. Second, there are the reactions of others as the story of the move is recounted; to some extent, the move is evaluated in terms of whether or not it was "worth it" – especially if the move was temporary or involved crossing states multiple times. At the first level, Medicaid HCBS users are able to tell their own stories and determine progress toward success on their own terms, while at the second, success is judged by others and involves a different set of indicators.
Given that none of the three examples discussed in this paper resulted in a successful cross-state move, they provide little guidance on this part of the model. However, the frustrated moves detailed above offer an important sort of "negative case" in which they illustrate a key utility of the model that might otherwise be missed. When moves, particularly those driven by opportunity (e.g., Volion, Murinko), are not undertaken then these trajectories are mapped using only the impetus for the move and the ability to move and the intrapersonal and interpersonal negotiations between these two. It is here that the embodied experiences of confinement within the state are illuminated and become apprehensible, an experience that typifies intrastate confinement.
Instrastate Confinement
Intrastate confinement is a concept that clarifies how the geopolitical boundaries that demarcate states can act to "wall in" marginalized people who try to cross these boundaries. Recognizing the state-boundedness of rights (e.g., ability to access HCBS) leads to an acknowledgement that crossing boundaries may lead to different, and often reduced, experiences of citizenship. The risk associated with constrained citizenship experienced by Medicaid HCBS users can act as a magnetic force to keep people in place, despite a strong desire to move. Consequently, individuals feel limited in their ability to move across state lines even when enticed to do so by the promise of educational, economic, or social advancement.
Influence of move story
Beyond the move itself, the stories told about the move have the potential to influence others in terms of both their willingness to pursue a move or to avoid such an endeavor.
Specifically, these stories are important resources that travel through social networks as HCBS users are self-assessing their ability to engage in a cross-state move. This is akin to how high school students evaluate potential schools by listening to stories from people who attend, or, indirectly, from others as they tell stories about those who have attended. For Medicaid HCBS users considering a cross-state move, stories of successful moves might act as encouragement, while stories of moves that were not successful may serve as cautionary tales or as narratives to be challenged by defying the odds. In the era of social media, stories circulate quickly and widely. The internet has been a particularly fertile arena for disability community and organizing; therefore, the potential influence of communication via these technologies is not to be underestimated and is another area that deserves attention from researchers.
Discussion
Barriers to cross-state movement for disabled people in the US are a social problem and would benefit from research that engage in a social problems analytic. The handful of existing studies that might identify and address this problem are methodologically and theoretically limited. For example, the Graefe et al. (2006) study does not include disabled people who were living independently and seeking employment, or those moving to leave their family of origin. Analyses of survey data on the reasons why people moved generally do not include comparisons by disability status. Although one survey about motivations for moving offered "health reasons" as a response, there were no options for moving closer to a family member to receive care, services, or supports, or conversely, to move closer to a family member who needs care, services, or supports (Ihrke 2014). Additionally, the quantitative nature of these studies does not allow for an exploration of the personal motivations for, or experiences of, those who moved, nor what these moves mean to individuals or families (Ihrke 2014; Ihrke and Faber 2012; Sharma 2011, 2013). These studies also fail to provide a means through which to assess the role of state-level policies in the decision-making processes on when, how, and where to move. Further, they do not address the meaning of these moves for society at large: what does it mean to have (or not have) data on the cross-state trajectories of individuals with disabilities? What does it mean that there are likely disparities in cross-state moves by disability status? What societal losses occur from these disparities? How do these disparities reflect an ableist lack of imagination about potential futures for disabled people, especially on the part of those who design and implement social policy? How do these disparities inform an understanding of justice and civil rights?
Moves in Context attends to how a cross-state move is influenced by a combination of social position/personal resources and structure/ideology. Thus, the model offers an opportunity to interpret and analyze a seemingly personal journey within the larger sociopolitical context (Mills 1959). The elements of the Moves in Context model were generated from stories of the experiences of actual disabled Medicaid HCBS users and were selected to demonstrate the agency of disabled people. They are intended to clarify how the futures desired by disabled people are supported or stymied by their personal resources and/or by their experiences of social structure (Kafer 2013). Furthermore, while intrastate confinement emerged from the model, naming the social and material consequences of these barriers to cross-state movement for disabled people, it holds the potential for broader application across a variety of situated experiences. Along with the model, the concept of intrastate confinement, have implications for future theoretical scholarship and empirical research on disability, citizenship, and mobility.
Moves in Context: A Tool for Future Research and Social Change
Moves in Context provides a tool through which to interrogate the socially situated experiences of cross-state movement for disabled people in the U.S. Future research must examine the ways in which Medicaid HCBS users pursue moves, how they define success in this process, and how move trajectories differ based on elements of the model (e.g., the impetus for moving). Specifically, investigating how individual HCBS users' moves influence others will afford an opportunity to explore how disabled people, their social networks, and their family members access and share information to assist others as they plan or start a cross-state move. The influence of one person's move might indeed impact the impetus to move for another.
Using the model to chart the cross-state movement trajectories of Medicaid HCBS users provides an opportunity to explore the unique patterns of experience within and across multiple populations. Drawing on the examples highlighted above, Zach Sayne represents one set of experiences while Shawn Murinko and Ashley Volion reflect quite another. Zach's story is about a child who becomes an adult, while both Shawn and Ashley are adults as they pursue moves. Zach's move is intimately tied to his role as son, and therefore, his mother is part of the determination of his journey; Ashley is making decisions as a single woman while, as a father and husband, Shawn's decisions impact his entire family. As a model, Moves in Context offers a prism through which to examine multiple disability experiences, preserving distinctions and inviting comparisons.
In addition to documenting barriers to cross-state movement, Moves in Context has the potential to chart how Medicaid HCBS users engage in cross-state moves, filling a gap in the literature. By examining successful cross-state moves, future research can identify common elements that facilitate moves and provide ideas for program development and policy change. Research can also address how individuals who pursue cross-state moves access information, receive personal care support during times of transition, and arrange for their personal care attendant services in a new place. Each of these areas could be used to develop and test an intervention to increase the likelihood of a successful cross-state move. Further, this data could be used in drafting new versions of the Disability Integration Act, Medicaid HCBS 1915(c) waivers, 1115 demonstration projects, or Money Follows the Person or Community First Choice provisions, justifying the inclusion of resources to help program users pursue cross-state moves.
Exploring the Broader Utility of Intrastate Confinement
In addition to charting individual program users' cross-state move trajectories, the Moves in Context model offers new vocabulary to document experiences of intrastate confinement of disabled people - where users find that due to differences in Medicaid HCBS offerings across states they are "stuck" in their current state, despite a desire to move elsewhere. Intrastrate confinement, however, has the potential to be applied much more broadly. It can be operationalized more generally as a social process of geographic immobility resulting from policy variations across locations (i.e., interstate variation) that (re)produce unequal and disparate experiences of citizenship for groups united by distinct characteristics (e.g., identity, program participation). Specifically, intrastate confinement manifests after an individual engages in reasoned consideration of how benefits and protections present in the current state would be forfeited, removed, or lessened by relocation. It is, therefore, produced through barriers to cross-state movement.
Intrastate confinement acknowledges that marginalized peoples are aware of how variations in state policies affect their access to State protections of economic stability and rights, and that cross-state moves may be accompanied by a loss of state-supported access to services, or antidiscrimination policies that offer protection in the areas of employment, housing, social services, and freedom from interpersonal and structural violence. As a result, intrastate confinement can be a useful concept for future sociological research on the effects of interstate variation in American social policy on the cross-state move patterns of: a) people of color (in relation to police misconduct, municipal responses to immigrant status, or voter suppression); b) lesbian and gay married couples (in relation to state laws that legalize discrimination); c) single women of reproductive age (in relation to abortion or contraceptive access); d) trans people (in relation to antidiscrimination policies, bathroom bills, state identification policies, and access to trans healthcare services and health insurance coverage); and e) lesbian, gay, bisexual and/or trans people (in relation to employment and/or housing antidiscrimination).
To close, the individual experiences of Medicaid HCBS users attempting to pursue cross-state moves are embedded within larger social contexts that are ripe for investigation and research, despite previous theoretical and empirical neglect. Engaging barriers to cross-state movement for disabled people as a social problem acknowledges the educational, employment, and social futures that Medicaid HCBS users (and more broadly, disabled people) imagine for themselves. It also examines the patterned ways in which these futures are facilitated or frustrated through variations in social policy and the ableist assumptions of those who design and implement policy. By undertaking this agenda, future research can produce knowledge to influence policy and advance equity for disabled people.
Acknowledgments
I would like to acknowledge the work of the anonymous reviewers and the editorial staff at DSQ whose suggested revisions helped improve this paper. I am grateful to Drs. Julia Rivera Drew, Carroll Estes, Richard Scotch, Allison Carey, and Glenn Fujiura for their feedback on earlier drafts of this manuscript and to Doron Dorfman for his encouragement on this project. Thank you to Jamie Cohn-Stacey for his dedicated editorial support in the preparation of this manuscript.
References
- 28 C.F.R. §35.130(d). 1998.
- ADAPT. 2018. Riding the wave of additional endorsements ADAPT urges Congress to pass Disability Integration Act. Retrieved May 21, 2018, from http://adapt.org/press-release-riding-wave-of-additional-endorsements-adapt-urges-congress-to-pass-disability-integration-act/
- Aisch, Gregor, Robert Gebeloff, and Kevin Quealy. 2014. "Where We Came from and Where We Went, State by State." The New York Times, August 14. Retrieved January 31, 2017 (https://www.nytimes.com/interactive/2014/08/13/upshot/where-people-in-each-state-were-born.html).
- Albrecht, Gary L. 1992. The Disability Business: Rehabilitation in America. SAGE Publications.
- Anon. 2017a. "H.R. 1628, Better Care Reconciliation Act of 2017." Congressional Budget Office. Retrieved July 27, 2017 (https://www.cbo.gov/publication/52849).
- Anon. 2017b. "H.R.1628 - 115th Congress (2017-2018): American Health Care Act of 2017." Retrieved July 28, 2017 (https://www.congress.gov/bill/115th-congress/house-bill/1628).
- Barnartt, Sharon N. and Richard K. Scotch. 2001. Disability Protests: Contentious Politics 1970-1999. Gallaudet University Press.
- Baynton, Douglas C. 2001. "Disability and the Justification of Inequality in American History." Pp. 33–57 in The New Disability History: American Perspectives, edited by P. K. Longmore and U. Umansky. New York, NY: New York University Press.
- Burwell, Sylvia Matthews. 2015. Community First Choice: Final Report to Congress. Washington, DC. Retrieved (https://www.medicaid.gov/medicaid/hcbs/downloads/cfc-final-report-to-congress.pdf).
- Caldwell, Joe. 2007. "Experiences of Families with Relatives with Intellectual and Developmental Disabilities in a Consumer-directed Support Program." Disability & Society 22(6):549–62. https://doi.org/10.1080/09687590701560139
- Caldwell, Joe and Tamar Heller. 2007. "Longitudinal Outcomes of a Consumer-Directed Program Supporting Adults with Developmental Disabilities and Their Families" edited by S. J. Taylor. Intellectual and Developmental Disabilities 45(3):161–173. https://doi.org/10.1352/1934-9556(2007)45[161:LOOACP]2.0.CO;2
- Carey, Allison C. 2009. On the Margins of Citizenship. Temple University Press. Retrieved February 7, 2017 (https://muse.jhu.edu/book/9236).
- Cass, Noel, Elizabeth Shove, and John Urry. 2005. "Social Exclusion, Mobility and Access." The Sociological Review 53(3):539–55. https://doi.org/10.1111/j.1467-954X.2005.00565.x
- Christiansen, John B. and Sharon N. Barnartt. 2003. Deaf President Now!: The 1988 Revolution at Gallaudet University. Gallaudet University Press.
- Conway, Karen Smith and Jonathan C. Rork. 2011. "The Changing Roles of Disability, Veteran, and Socioeconomic Status in Elderly Interstate Migration." Research on Aging 33(3):256–85. https://doi.org/10.1177/0164027511399107
- Eiken, Steve, Kate Sredl, Brian Burwell, and Paul Saucier. 2015. Medicaid Expenditures for Long-Term Services and Supports (LTSS) in FY 2013. United States Department of Health and Human Services, Centers for Medicare & Medicaid Services. Retrieved February 7, 2017 (https://www.medicaid.gov/medicaid/ltss/downloads/ltss-expenditures-fy2013.pdf).
- Eiken, Steve, Kate Sredl, Brian Burwell, and Paul Saucier. 2016. Medicaid Expenditures for Long-Term Services and Supports (LTSS) in FY 2014: Managed LTSS Reached 15 Percent of LTSS Spending. United States Department of Health and Human Services, Centers for Medicare & Medicaid Services. Retrieved (https://www.medicaid.gov/medicaid/ltss/downloads/ltss-expenditures-2014.pdf).
- Fleischer, Doris Zames and Frieda Zames. 2011. The Disability Rights Movement: From Charity to Confrontation. Updated ed. Philadelphia: Temple University Press.
- Graefe, Deborah Roempke, Gordon F. De Jong, and Dee C. May. 2006. "Work Disability and Migration in the Early Years of Welfare Reform." Population Research and Policy Review 25(4):353–68. https://doi.org/10.1007/s11113-006-9001-x
- Grossman, Brian R. 2011. "Same Mandate, Changing Concepts of Community: An Analysis of Bills to Mandate Medicaid Coverage of Community-Based Attendant Services and Supports (1997–2010)." Pp. 215–40 in Research in Social Science and Disability, vol. 6, edited by A. C. Carey and R. K. Scotch. Emerald Group Publishing Limited. Retrieved February 1, 2017. https://doi.org/10.1108/S1479-3547(2011)0000006012
- Grossman, Brian R., Martin Kitchener, Joseph T. Mullan, and Charlene Harrington. 2007. "Paid Personal Assistance Services." Journal of Aging & Social Policy 19(3):27–45. https://doi.org/10.1300/J031v19n03_03
- Hahn, Harlan. 1988. "The Politics of Physical Differences: Disability and Discrimination." Journal of Social Issues 44(1):39–47. https://doi.org/10.1111/j.1540-4560.1988.tb02047.x
- Hughes, Bill and Kevin Paterson. 1997. "The Social Model of Disability and the Disappearing Body: Towards a Sociology of Impairment." Disability & Society 12(3):325–40. https://doi.org/10.1080/09687599727209
- Ihrke, David K. 2014. Reasons for Moving: 2012 to 2013. Washington, DC: United States Census Bureau. Retrieved February 7, 2017 (http://www.census.gov/prod/2014pubs/p20-574.pdf).
- Ihrke, David K. and Carol S. Faber. 2012. Geographic Mobility: 2005 to 2010. Washington, DC: United States Census Bureau. Retrieved February 7, 2017 (https://www.census.gov/prod/2012pubs/p20-567.pdf).
- Ingraham, Christopher. 2015. "[Graphic of State Migration Flow Data from the American Community Survey 2012] State Migration Flows, 2012." Retrieved February 7, 2017 (http://bl.ocks.org/cingraham/7663357).
- Kafer, Alison. 2013. Feminist, Queer, Crip. Bloomington, IN: Indiana University Press.
- Kassner, Enid et al. 2008. A Balancing Act: State Long-Term Care Reform. AARP, Public Policy Institute Washington, DC. Retrieved February 8, 2017 (http://globalag.igc.org/health/us/2008/longtermcare.pdf).
- Kassner, Enid and Lee Shirey. 2000. Medicaid Financial Eligibility for Older People: State Variations in Access to Home and Community-Based Waiver and Nursing Home Services. AARP Public Policy Institute Washington, DC. Retrieved February 7, 2017 (https://assets.aarp.org/rgcenter/health/2000_06_medicaid.pdf).
- Katz, Sidney, Thomas D. Downs, Helen R. Cash, and Robert C. Grotz. 1970. "Progress in Development of the Index of ADL." The Gerontologist 10(1_Part_1):20–30.
- Kaye, H.Stephen, Charlene Harrington, and Mitchell P. LaPlante. 2010. "Long-Term Care: Who Gets It, Who Provides It, Who Pays, and How Much?" Health Affairs 29(1):11–21. https://doi.org/10.1377/hlthaff.2009.0535
- Kitchener, Martin, Terence Ng, and Charlene Harrington. 2007. "Medicaid Home and Community-Based Services for the Elderly: Trends in Programs and Policies." Journal of Applied Gerontology 26(3):305–24. https://doi.org/10.1177/0733464807302135
- LaPlante, Mitchell P., H.Stephen Kaye, Taewoon Kang, and Charlene Harrington. 2004. "Unmet Need for Personal Assistance Services: Estimating the Shortfall in Hours of Help and Adverse Consequences." The Journals of Gerontology: Series B 59(2):S98–108.
- Lawton, M.Powell and Elaine M. Brody. 1969. "Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living." The Gerontologist 9(3_Part_1):179–86.
- LeBlanc, Allen J., M.Christine Tonner, and Charlene Harrington. 2000. "Medicaid 1915(c) Home and Community-Based Services Waivers across the States." Health Care Financing Review; Washington 22(2):159–74.
- Leiter, Valerie. 2012. Their Time Has Come: Youth with Disabilities on the Cusp of Adulthood. New Brunswick, N.J: Rutgers University Press.
- Liachowitz, Claire H. 1988. Disability as a Social Construct: Legislative Roots. University of Pennsylvania Press.
- Lipsky, Michael. 1983. Street Level Bureaucracy: Dilemmas of the Individual in Public Services. New York: Russell Sage Foundation.
- Litwak, Eugene and Charles F. Longino. 1987. "Migration Patterns among the Elderly: A Developmental Perspective." The Gerontologist 27(3):266–72. https://doi.org/10.1093/geront/27.3.266
- Marshall, Thomas H. 1950. "Citizenship and Social Class." in The Welfare State Reader, vol. 11. Cambridge. Retrieved February 7, 2017 (https://books.google.com/books?hl=en&lr=&id=kSwy6f0PghMC&oi=fnd&pg=PA30&dq=Citizenship+and+Social+Class&ots=bDKDV2gecH&sig=YhFo2sKZ0ONHuneEuJbB3hA5KX8).
- Mason, Betsy. 2013. "Mapping America's Restless Interstate Migration without a Map." WIRED. Retrieved February 13, 2017 (https://www.wired.com/2013/11/mapping-migration-without-a-map/).
- Mateyka, Peter J. 2015. Desire to Move and Residential Mobility. Washington, DC: United States Census Bureau. Retrieved February 7, 2017 (https://www.census.gov/content/dam/Census/library/publications/2015/demo/p70-140.pdf).
- Mills, C.Wright. 1959. The Sociological Imagination. Oxford University Press.
- Murinko, Shawn. 2014. "Held down by red tape, not disability." TheHill. Retrieved February 7, 2017 (http://thehill.com/blogs/congress-blog/civil-rights/208381-held-down-by-red-tape-not-disability).
- NCIL. 2018. About visitability. Retrieved May 21, 2018, from https://visitability.org/about-visitability/
- Ng, Terence, Charlene Harrington, MaryBeth Musumeci, and Petry Ubri. 2016. Medicaid Home and Community-Based Services Programs: 2013 Data Update. The Kaiser Commission on Medicaid and the Uninsured. Retrieved February 7, 2017 (http://files.kff.org/attachment/Report-Medicaid-Home-and-Community-Based-Services-Programs-2013-Data-Update).
- Nielsen, Kim E. 2012. A Disability History of the United States. Paperback edition. Boston: Beacon Press.
- O'Connor, James. 1973. The Fiscal Crisis of the State. 4th ed. Piscataway, NJ.
- O'Rand, A. M. 1996. "The Precious and the Precocious: Understanding Cumulative Disadvantage and Cumulative Advantage over the Life Course." The Gerontologist 36(2):230–38. https://doi.org/10.1093/geront/36.2.230
- Offe, Claus. 1984. Contradictions of the Welfare State. Cambridge, MA: MIT Press.
- Office of the Secretary, Department of Health and Human Services. 2015. Federal Financial Participation in State Assistance Expenditures; Federal Matching Shares for Medicaid, the Children's Health Insurance Program, and Aid to Needy Aged, Blind, or Disabled Persons for October 1, 2016 Through September 30, 2017.
- Oliver, Michael. 1983. Social Work with Disabled People. Macmillan. https://doi.org/10.1007/978-1-349-86058-6
- Oliver, Michael and Colin Barnes. 2012. The New Politics of Disablement. Palgrave Macmillan.
- Olmstead v. L. C. 527 U.S. 581 (1999).
- Pelka, Fred. 2012. What We Have Done: An Oral History of the Disability Rights Movement. Amherst: University of Massachusetts Press.
- Reinhard, Susan C. et al. 2014. Raising Expectations: A State Scorecard on Long-Term Services and Supports for Older Adults, People with Physical Disabilities, and Family Caregivers.
- Reinhard, Susan C., Enid Kassner, Ari Houser, and Robert Mollica. 2011. Raising Expectations: A State Scorecard on Long-Term Services and Supports for Older Adults, People with Physical Disabilities, and Family Caregivers. Retrieved January 31, 2017 (https://www.aucd.org/docs/policy/health_care/ltss_scorecard.pdf).
- Ruiz, Lorena. 2013. "Louisiana, Not Cerebral Palsy, Deferring Woman's Ph.D. Dream." MSNBC. Retrieved February 7, 2017 (http://www.msnbc.com/melissa-harris-perry/louisiana-not-cerebral-palsy-deferring-woma).
- Russell, Marta. 1998. Beyond Ramps: Disability at the End of the Social Contract: A Warning from an Uppity Crip. Common Courage Press.
- Ryan, Paul. 2016. A Better Way: Our Vision for a Confident America - Health Care. Retrieved (http://abetterway.speaker.gov/_assets/pdf/ABetterWay-HealthCare-PolicyPaper.pdf).
- San Antonio, Patricia et al. 2009. "Lessons From the Arkansas Cash and Counseling Program: How the Experiences of Diverse Older Consumers and Their Caregivers Address Family Policy Concerns." Journal of Aging & Social Policy 22(1):1–17. https://doi.org/10.1080/08959420903385544
- Schumer, Charles. 2017. "S.910 - 115th Congress (2017-2018): Disability Integration Act of 2017." Retrieved July 28, 2017 (https://www.congress.gov/bill/115th-congress/senate-bill/910).
- Schwalbe, Michael. 2007. The Sociologically Examined Life: Pieces of the Conversation. McGraw-Hill Education.
- Schweik, Susan M. 2010. The Ugly Laws: Disability in Public. NYU Press.
- Scotch, Richard. 2009. From Good Will to Civil Rights: Transforming Federal Disability Policy. Temple University Press.
- Scott, Robert A. 1981. The Making of Blind Men. 1 edition. New Brunswick, N.J: Routledge.
- Shapiro, Isaac, Bryan DaSilva, David Reich, and Richard Kogan. 2016. Funding for Housing, Health, and Social Services Block Grants Has Fallen Markedly over Time. Retrieved (http://www.cbpp.org/sites/default/files/atoms/files/11-19-15bud.pdf).
- Shapiro, Joseph. 2013. "Why a Young Man Died in a Nursing Home, a State Away from His Mom." NPR.org. Retrieved February 7, 2017 (http://www.npr.org/sections/health-shots/2013/01/15/169457118/why-a-young-man-died-in-a-nursing-home-a-state-away-from-his-mom).
- Sharma, Andy. 2011. "Selective out-Migration from Florida." Population Research and Policy Review 30(6):817–38. https://doi.org/10.1007/s11113-011-9212-7
- Sharma, Andy. 2013. "The Chain Is Only as Strong as the Weakest Link: Older Adult Migration and the First Move." Research on Aging 35(5):507–532. https://doi.org/10.1177/0164027512446836
- Sherry, Mark. 2016. "A Sociology of Impairment." Disability & Society 31(6):729–44. https://doi.org/10.1080/09687599.2016.1203290
- Simon-Rusinowitz, L. et al. 2001. "Consumer and Surrogate Preferences for a Cash Option versus Traditional Services: Florida Adults with Developmental Disabilities." Mental Retardation 39(2):87–103. https://doi.org/10.1352/0047-6765(2001)039<0087:CASPFA>2.0.CO;2
- Solomon, Judith. 2017. Existing Medicaid Flexibility Has Broadened Reach of Home- and Community-Based Services, Testimony of Judith Solomon Vice President, Center on Budget and Policy Priorities Before the Health Subcommittee of the House Energy and Commerce Committee. Retrieved (http://www.cbpp.org/health/existing-medicaid-flexibility-has-broadened-reach-of-home-and-community-based-services).
- Stone, Deborah. 1984. The Disabled State. Philadelphia: Temple University Press.
- Summer, Laura and Emily S. Ihara. 2005. The Medicaid Personal Care Services Benefit: Practices in States That Offer the Optional State Plan Benefit. AARP, Public Policy Institute. Retrieved February 7, 2017 (http://assets.aarp.org/rgcenter/health/2005_11_medicaid.pdf).
- Thomas, Carol. 2004. "How Is Disability Understood? An Examination of Sociological Approaches." Disability & Society 19(6):569–83. https://doi.org/10.1080/0968759042000252506
- United States Census Bureau. 2015. "[Excel Spreadsheet of American Community Survey Data on Cross-State Moves] State-to-State Migration Flows: 2015." Retrieved (http://www2.census.gov/programs-surveys/demo/tables/geographic-mobility/2015/state-to-state-migration/State_to_State_Migrations_Table_2015.xls).
- Urry, John. 2000a. "Mobile Sociology." British Journal of Sociology 51(1):185–203.
- Urry, John. 2002. "Mobility and Proximity." Sociology 36(2):255–74. https://doi.org/10.1177/0038038502036002002
- Urry, John. 2000b. Sociology beyond Societies: Mobilities for the Twenty-First Century. Routledge.
- Wenzlow, Audra, Rosemary Borck, Dean Miller, Pamela Doty, and John Drabek. 2013. An Investigation of Interstate Variation in Medicaid Long-Term Care Use and Expenditures across 40 States in 2006. Washington, DC: United States Department of Health and Human Services, Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy. Retrieved January 31, 2017 (https://aspe.hhs.gov/sites/default/files/pdf/76906/40State.pdf).
Endnotes
-
Institutional bias refers to uneven distribution of Medicaid dollars toward nursing homes (and other institutions) over community living options. In 2012, the percentage of Medicaid dollars spent on community living was nearly equal to that spent on institutions for the first time since the introduction of HCBS waivers in 1981 (Eiken et al. 2016).
Return to Text
